


Managing Infection in Contact Lens Wearers
BY GREGORY J. NIXON, O.D.
FEBRUARY 1998
When ocular infection strikes, your patients rely upon you to restore their eye health and get them back into contact lenses. Are you up to the task?
Most contact lens patients achieve great success and enjoy all the benefits of contact lenses without encountering serious infection. However, the application of a contact lens to the eye can introduce additional risks for ocular infection. While ocular infection is not limited to contact lens wearers, they often have a higher microbial concentration within the precorneal tear film. Corneal epithelial defects secondary to contact lens induced mechanical trauma, hypoxic stress or desiccation can create a site for opportunistic microbial invasion. Nonetheless, complications are most common in extended wear or cases of patient noncompliance including poor personal hygiene, lens overwear and neglect of proper lens replacement schedules, cleaning regimens and follow-up appointments. So when infection does occur, proper care means not only treating the infection but also addressing lens-related issues such as wearing schedules and care system compliance. The following review of the differential diagnosis and management strategies for ocular infections in contact lens wearers will help familiarize you with this increasingly relevant aspect of primary eye care.
Bacterial Infection
Conjunctivitis -- The immune response to bacterial infection is dominated by the neutrophilic white blood cells. Neutrophil activation results in papillary hypertrophy of the palpebral conjunctiva (multiple small tissue elevations with a pinpoint vessel in the center) and mucopurulent discharge (Fig. 1). In the absence of corneal infection, meaty red injected conjunctival blood vessels present with increasing redness toward the fornices. A patient will typically complain of a unilateral red eye and burning, a foreign body sensation or mild ocular discomfort. Due to the mucopurulent discharge, patients will often complain that their eyes are stuck together upon awakening.

FIG. 1: Bacterial conjunctivitis
Although these infections are often self-limiting and are resolved by the immune system alone, the use of topical antibiotics can often expedite recovery and prevent the infection from getting worse. A broad-spectrum antibiotic solution such as Polytrim (t.i.d.) or tobramycin (q.i.d.) is the treatment of choice. Continue treatment for at least seven days and for two to three days after the infection resolves to prevent recurrence. If a patient presents with rapid onset and progression within 12 to 24 hours of symptoms, as well as with signs of a severe inflammatory reaction including lid swelling, marked bulbar conjunctival chemosis, creamy white purulent discharge and preauricular lymphadenopathy (PAL), suspect a hyperacute conjunctivitis. This presentation can indicate a gonococcal infection, which is capable of penetrating an intact cornea. Swift and immediate management is essential, starting with culture and sensitivity testing. Treatments vary according to lab results but often require hospitalization for intravenous or intramuscular cephalosporins in addition to topical fluoroquinolone therapy.
Keratitis -- Infection of the cornea by an opportunistic microbe provokes a compelling clinical presentation. Although the cornea is an avascular tissue, the surrounding limbal vasculature actively provides immunological protection against antigenic substances. These limbal vessels are often prominent in contact lens wearers, especially extended lens wearers, due to hypoxic stress resulting from decreased diffusion of the atmospheric oxygen necessary to fuel the cornea's metabolic processes. Antigenic recognition of microbes that have penetrated the corneal epithelium triggers a cascade of biochemical events, causing antibodies, inflammatory mediators and white blood cells to migrate from the limbal vessels to the site of infection. The conglomeration of white blood cells together form a corneal infiltrate. The tissue destruction secondary to proliferating microbes and inflammatory cells can cause necrosis of the surrounding and overlying tissue. A corneal infiltrate with an overlying epithelial defect defines a corneal ulcer.
Until proven otherwise, assume that the presence of central or midperipheral corneal infiltrates without an overlying epithelial defect in a contact lens wearer is infectious. It's likely that this presentation is in a pre-ulcer stage, where the epithelium has not yet become necrotic. In a full-blown infectious corneal ulcer (Fig. 2), the infiltrative corneal lesion is characterized by a well-excavated epithelial defect that will stain intensely. A moderate to severe anterior chamber reaction can be present with 2 to 4+ cells and/or flare and possible hypopyon formation. The acute onset of the profound inflammatory reaction causes patients to be very symptomatic, complaining of profuse tearing, marked redness, pain, intense photophobia and sometimes a decrease in vision.
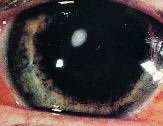
FIG. 2: Infectious keratitis.
Some infectious agents can cause rapid destruction of tissue and can perforate the cornea. For this reason, perform culture and sensitivity testing for lesions within the central six millimeters of the cornea to ensure that the initial antimicrobial therapy targets the offending organism. Many practitioners may choose to treat lesions outside the central six millimeters with broad spectrum antibiotics and pursue culturing if no response to treatment occurs. It's recommended to refer lesions that impinge on the visual axis to a corneal specialist.
The hallmark treatment of a bacterial corneal ulcer includes a regimen of topical fortified antibiotics (cefazolin and gentamycin or tobramycin). Recently, studies have shown that a 0.3% fluoroquinolone (Ciloxan or Ocuflox) used as a stand-alone medication is equally effective. Advantages to prescribing a fluoroquinolone versus fortified antibiotics include widespread availability, ready-to-use formulation and possible improved patient compliance due to less bottle confusion and less burning and stinging upon instillation. The recommended fluoroquinolone dosage is two drops every 15 minutes for six hours, two drops every 30 minutes for 18 hours, then two drops every one to two hours for the next 24 to 48 hours based on follow-up evaluation. In addition to antibiotics, topical cycloplegics and oral analgesics help relieve discomfort. Reports of fluoroquinolone resistance highlight the value of culture and sensitivity testing at the initial presentation. If a 24-hour follow-up visit shows progression, perform additional cultures to detect viral, fungal or protozoan infection as well as bacterial resistance.
Noninfectious Keratitis -- Not all corneal ulcers are infectious. Relatively small (<2.0mm) lesions that inhabit the peripheral cornea and leave an area of clear cornea between the lesion and the limbus are typically caused by an immune hypersensitivity. The antigens typically responsible for triggering the immune response are exotoxins from staphylococcal organisms. This normal bacterial flora may be present in high concentration secondary to active lid disease, adherence to the contact lens or stagnation of the tear film behind the lens. Unlike an infectious ulcer, there's usually minimal to no patient symptoms, minimal to no anterior chamber reaction and mild to moderate staining over the lesion.
Management may include antibiotic therapy to decrease microbial concentration and serve as prophylaxis against infection at the sight of the epithelial defect. Common therapies include the use of Polytrim or a topical fluoroquinolone solution every four hours while awake and an antibiotic ointment (Polysporin or erythromycin) applied to the lid margin at bedtime and up to three times a day Some practitioners manage the inflammatory response directly with a topical steroid or antibiotic/steroid combination, but to best guard against infection in the cornea's compromised state, prescribe a stand-alone antibiotic initially, adding a steroid if the immune response persists. Educate patients on the nature of the problem, and instruct them to regularly perform hot compresses and lid scrubs to improve hygiene and limit staphylococcal overgrowth.
Viral Infection
Non-herpetic Conjunctivitis -- The immune response to a viral infection is mediated primarily by the lymphocytic white blood cells. The lymphocyte inflammatory response results in palpebral conjunctival follicles, which appear as large, translucent elevations surrounded at the base by palpebral vessels. Other ocular signs include a thin, watery discharge, diffuse pinkish conjunctival injection, and possibly small pinpoint conjunctival or subconjunctival hemorrhages (Fig. 3). Patients will often have the awareness of redness and watering as their only symptoms. Onset may coincide with or follow a cold or upper respiratory infection.

FIG. 3: Viral conjunctivitis.
Viral infections are highly contagious and often progress from one eye to the other in a matter of days. Instruct patients to wash their hands frequently, to avoid touching their eyes and to avoid sharing personal items (towels, make-up, etc.). Although new nonspecific antiviral agents are being studied, none are currently approved for therapeutic use. Current treatments are mostly palliative measures used until the condition runs its course. Artificial tears used four to eight times a day may improve surface irritation and dilute viral concentration. A topical vasoconstrictor such as Naphcon-A or Opcon-A used four times a day can decrease conjunctival redness.
Non-herpetic Keratitis -- Some adenoviruses (especially types 8 and 19) can infect the cornea, resulting in epidemic keratoconjunctivitis (EKC). The corneal signs will typically develop seven to 10 days after the initial onset of conjunctival involvement (injection, follicles, watery discharge). Multiple, diffuse subepithelial corneal infiltrates that don't stain will develop and can persist for one to four weeks. Infiltrates lying on the visual axis can decrease visual acuity and hamper visual function. Like non-herpetic conjunctivitis, there is currently no direct antiviral treatment. Topical steroids (FML or Pred Mild q.i.d. for one week) may help diminish corneal infiltrates and improve vision, but a recurrence of signs and symptoms often follows after the steroid taper. Therefore, most cases of EKC are managed with the palliative treatments already discussed above.
FIGURE 1:
|
||||||||||||||||||
Herpes Simplex Conjunctivitis -- It is estimated that over 90 percent of humans have been exposed to and carry the herpes simplex virus. In most immunocompetent patients, the virus does not proliferate and cause active infection. Patients with challenges to their immune system from fatigue, stress, a present illness or immunocompromise from chronic disease or medication are predisposed to infection.
The ocular signs are similar to those of a non-herpetic conjunctivitis, except that it is a strictly unilateral phenomenon. There may also be clear dermatologic vesicles on the lid or periorbital skin that progress to form crusty lesions. In contrast to non-herpetic lesions, there are FDA-approved antiviral medications available for treatment of herpetic lesions. In the absence of corneal involvement, topical 1% trifluorothymidine (Viroptic) solution or 3% vidarabine ointment (Vira-A) is indicated five times a day. Viroptic must be refrigerated to maintain its effectiveness. Continue treatment for seven to 14 days after resolution due to an extremely high recurrence rate. Treat skin lesions with warm soaks and erythromycin or acyclovir ointment, although acyclovir is expensive and its effectiveness is questionable.
Herpes Simplex Keratitis -- Corneal involvement with herpes simplex infection results in a dendritic ulceration of the corneal epithelium (Fig. 4). Fluoroscein or rose bengal stain will highlight end bulbs. Classically, the cotton wisp test will elicit a decrease in corneal sensitivity in the infected eye in comparison to the fellow eye.

FIG. 4: Dendritic keratitis
A dendritic ulcer in the presence of a unilateral follicular conjunctivitis is pathognomonic of herpes simplex keratitis and does not require culturing before initiating treatment with Viroptic nine times a day in conjunction with Vira-A ointment instilled at bedtime. The high toxicity of antiviral medications limits their use to a course of 21 days. Most lesions will heal and resolve within this time frame, but if not, discontinue the antivirals because their toxic effects on the cornea may be preventing healing.
Fungal and Protozoan Infection
Managing fungal and protozoan corneal infection is not within the scope of primary eye care. Treatment protocols call for hospitalization and the use of both topical and systemic anti-infective therapy to minimize tissue destruction, scarring and loss of visual acuity. Though these cases are rare, it's critical that you be able to recognize these types of infection and provide expeditious referral for proper tertiary care.
Fungal infection is commonly caused by trauma to the eye with vegetable matter such as a tree branch. The corneal infiltrate takes on a gray, feathery appearance and often has small satellite lesions around the primary infiltrate. There is a profound inflammatory anterior chamber reaction often resulting in hypopyon formation.
Although the use of nonsterile homemade saline solutions is exceedingly rare today, the water-bound protozoan acanthamoeba, often present in swimming pools or hot tubs, is still a menacing cause of corneal infection particularly in soft lens wearers. Ocular presentation includes a painful red eye with multiple corneal infiltrates and little to no overlying epithelial disruption. Patients typically present with symptoms of excruciating pain that does not fit the clinical picture. At this stage, it is often misdiagnosed as a bacterial infection and antibiotic therapy is instituted. When not properly diagnosed, the disease progresses, causing the formation of the classic ring infiltrate (Fig. 5). So, when antibiotic therapy fails, take a culture and include Giemsa and calcofluor white stain in the lab tests.

FIG. 5: Acanthamoeaba keratitis
Chronic Conjunctivitis
There are occasions when a condition may fail to respond to initial treatment or even to a change in treatment. A condition that persists beyond a four-week duration is considered chronic and requires further investigation to uncover the true etiology.
For example, a chronic follicular conjunctivitis may be secondary to molluscum contagiosum. This condition is caused by a pox virus that forms a wart-like dermatologic lesion which sheds its viral components into the eye when the lesion is located on the lid or periorbital skin. Simple excision or cryosurgery of the lesion removes the offending virus and resolves the subsequent follicular conjunctivitis.
Systemic chlamydial infection, a sexually transmitted disease, can produce secondary ocular effects in the form of adult inclusion conjunctivitis. Inclusion conjunctivitis is considered a chronic condition because it is often initially misdiagnosed as a simple bacterial conjunctivitis and doesn't respond to topical antibiotic therapy alone. Presentation is characterized by a non-resolving red eye with conjunctival injection, a mixed papillary and follicular response, persistent mucous discharge, preauricular lymphadenopathy, superior pannus and variable tiny subepithelial infiltrates in the superior aspect of the cornea. When suspicious of inclusion conjunctivitis, explore the presence of concomitant systemic conditions like vaginitis or urethritis. Ask whether the patient has experienced any genital discharge or pain with urination. A medical evaluation by a physician or lab studies showing basophilic intracytoplasmic inclusion bodies from a conjunctival scraping with a Giemsa stain will often confirm the diagnosis. Treatment includes tetracycline or erythromycin (250mg p.o. q.i.d.) or doxycycline (100mg p.o. b.i.d. ) for three to four weeks. Topical therapy includes tetracycline ointment (Achromycin) or erythromycin ointment (Ilotycin) three times a day for two to three weeks. The patient and sexual partners should be treated and encouraged to seek medical evaluation to detect other sexually transmitted diseases.
Management PearlsAlthough each case requires an individualized therapeutic treatment, there are some universal clinical pearls that apply to all infection management protocols for contact lens patients.
Each case of ocular infection requires an appropriate follow-up schedule until resolution of the condition. Due to the progressive and sometimes unpredictable nature of some opportunistic microbes, instruct all patients being treated for an infection to seek care immediately if their symptoms worsen. |
