


Unmasking the RGP Fit With Fluorescein
TOmitting fluorescein pattern evaluation from the RGP fitting process could leave you in the dark. Here's how this simple technique can light your way to optimum lens selection.
BY EDWARD S. BENNETT, OD, MSEd, JOSEPH T. BARR, OD, MS, EDITOR &
JEFFREY JOHNSON, OD
OCTOBER 1998
One of the great misperceptions about rigid gas permeable (RGP) contact lenses is that they are difficult to fit. Actually, nothing could be further from the truth, especially when following this three-fold approach to fitting: 1) presenting RGPs properly to the patient; 2) making the fitting as efficient as possible; and 3) carefully evaluating the lens-to-cornea relationship with fluorescein.
Proper presentation -- Patients need to know that they will experience some lens awareness during the adaptation period and be reassured that comfort should follow adaptation.
Efficient fitting -- To compete effectively with soft lenses, RGP fitting must not be too time-consuming. Certainly, instilling a topical anesthetic will reduce the initial apprehension in new wearers and therefore reduce the time needed to evaluate the lens. As Keith Ames, O.D., has emphasized, empirical fitting is another way to reduce initial chair time, provided that the practitioner obtains sufficient experience to feel proficient with the more routine RGP fits.
Fluorescein evaluation -- New graduates take it for granted that every rigid lens fit must be evaluated with fluorescein. However, this is typically one of the first shortcuts taken by practitioners who fit rigid lenses. It wouldn't be surprising if the number of practitioners who don't use fluorescein for rigid lens evaluation rivals the number of those who do. Here, we demonstrate why fluorescein application is the key to successful RGP contact lens fitting.
Fluorescein Instillation and Evaluation
Fluorescein is available in both liquid and impregnated paper strip forms; the latter is most commonly used for rigid contact lens evaluation. It's important to first clean the lenses using a rigid lens cleaner and to condition the lenses with a wetting solution. Wet the strip with an ophthalmic irrigating or buffered saline solution and shake off any excess solution prior to application. Have the patient look down and gently place the moistened strip against the superior conjunctiva. Advise the patient to blink several times and evaluate the fluorescein pattern once the lens rests prior to the next blink. It's important to evaluate the pattern in the horizontal and vertical meridians independently; likewise assess the pattern in the periphery of the lens.
You can use both a biomicroscope and a Burton lamp to evaluate the fluorescein pattern. Advantages of the biomicroscope include variable illumination and magnification, although low magnification and high illumination are recommended. Using a cobalt blue filter over the illumination system is required. In addition, using a yellow barrier filter (i.e., Wratten #12 or Tiffen #2) will result in greater fluorescence, especially with RGP lens materials that have ultraviolet blocking agents (Figs. 1a & 1b).
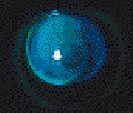
FIG. 1a: Fluorescein evaluation without a yellow filter. |

FIG. 1b: Fluorescein evaluation with a yellow filter. |
A Burton lamp, which is a handheld lamp with a +5.00D magnifier manufactured by Burton Medical Products, is also beneficial. Although magnification and illumination are not variable, this instrument is especially helpful when observing both eyes at once or when evaluating some of the more distinctive patterns, such as those in patients with high corneal toricity and keratoconus.
An alignment fitting relationship along the optical zone of the lens, which provides a thin, even layer of tear film between lens and cornea, is most desirable. A light green fluorescein pattern confirms this relationship. The periphery of the lens should show a slightly denser green color, representing greater edge clearance from the cornea, allowing tear exchange and preventing mechanical trauma to the cornea upon blinking (Fig. 2).

FIG. 2: Alignment fit pattern. |
Fluorescein pattern evaluation, which is fast and easy to perform, is also an essential confirmation test to ensure that an optimum lens-to-cornea fitting relationship exists. Assuming based upon good lens centration that an optimum, healthy fit is present can only result in lens-induced complications, as the following cases show.
Revealing Hidden Truths
CASE 1: High Corneal Eccentricity
Patient S.P., a 16-year-old female, wanted contact lenses for the first time. Her refractive data was as follows:
Manifest Refraction:
- OD: -3.75 - 1.25 x 173, 20/20
- OS: -3.50 - 1.00 x 005, 20/20
Keratometry:
- OD: 42.00 @ 180 / 43.00 @ 090 Mires Clear
- OS: 42.50 @ 180 / 43.25 @ 090 Mires Clear
Her pupil size OU was 5.0mm in normal room illumination and 7.5mm in dim illumination. While corneal topography revealed no irregularity, the corneal eccentricity was 0.62 OD and 0.61 OS.
S.P. is a progressive myope, so her practitioner recommended RGP lenses. S.P. was fit on K with the following diagnostic lenses:
| OD | OS | |
| BCR: | 8.04mm | 7.94mm |
| OAD/OZD: | 9.0/7.6mm | 9.0/7.6mm |
| Power: | -3.00D | -3.00D |
S.P. indicated that she experienced lens awareness but that the comfort was better than she had imagined. In addition, with an overrefraction of -0.75D OD and OS, her vision was 20/20+ in both eyes. Slit lamp evaluation revealed good centration, but upon instillation of fluorescein, an apical clearance or steep fitting relationship became apparent, as well as midperipheral bearing and insufficient peripheral clearance (Fig. 3). The lenses moved only about 0.5mm with the blink. After further diagnostic fitting, the following lenses were ordered:
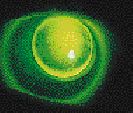
FIG. 3: Apical clearance pattern. |
| OD | OS | |
| BCR: | 8.18mm | 8.08mm |
| OAD/OZD: | 9.5/8.1mm | 9.5/8.1mm |
| Power: | -3.00D | -3.00D |
With these lenses, fluorescein evaluation showed an alignment fitting relationship accompanied by both good centration and movement.
This is an excellent example of how, without fluorescein application, it would be easy to be misled into thinking that S.P. has a good fitting relationship. Had she continued to wear lenses with the original base curve radii, it is likely that lens stagnation would have developed from a combination of apical clearance and limited peripheral clearance. There is a common misperception that on-K is equivalent to alignment in terms of fitting relationship. The cornea flattens toward its periphery and yet the base curve is spherical, so a lens typically needs to be fit 0.50D flatter than K to achieve an alignment fit, especially if the patient has a high rate of flattening (i.e., eccentricity).
In this case, a 0.50D flatter-than-K base curve radius produced an alignment fitting relationship. However, as a result of the fairly large pupil diameter, lenses 0.5mm larger were ordered. To maintain the same alignment fluorescein pattern, the final base curve radii were flattened an additional 0.25D.
CASE 2: High Corneal Astigmat
B.M., a 15-year-old male, wanted to wear contact lenses for the first time. His refractive data was:
Manifest Refraction:
- OD: -2.00 - 2.25 x 180, 20/20
- OS: -1.50 - 2.00 x 176, 20/20
Keratometry:
- OD: 42.00 @ 180 / 45.00 @ 090 Mires Clear
- OS: 41.50 @ 180 / 44.25 @ 090 Mires Clear
B.M. was fit with the following diagnostic lenses:
| OD | OS | |
| BCR: | 7.89mm | 8.04mm |
| OAD/OZD: | 9.2/7.8mm | 9.2/7.8mm |
| Power: | -3.00D | -3.00D |
Overrefraction:
- OD: +0.50 - 1.00 x 090, 20/20; +0.25DS; 20/25
- OS: +1.25 - 0.75 x 090, 20/20; +1.00DS; 20/25+1
Biomicroscopy revealed good centration OU. Upon instilling fluorescein, the dumbbell-shaped pattern shown in Figure 4 appeared. Therefore, Polycon SPE bitoric lenses were fit using the following diagnostic lenses:

FIG. 4: Spherical lens on a high corneal astigmat. |
| OD | OS | |
| BCR: | 41.50(8.13)/ 43.50(7.76) |
41.00(8.23)/ 43.00(7.85) |
| OAD/OZD: | 9.0mm | 9.0mm |
| Power: | PL/-2.00D | PL/-2.00D |
The overrefraction was as follows:
- OD: -0.50 - 1.00 x 090, 20/20+
- OS: -0.25 - 0.75 x 090, 20/20+
An alignment fluorescein pattern was achieved OU and the final lens powers were:
- OD: (-1.50 + PL)/-0.50 + (-)2.00 = -1.50/-2.50
- OS: (-1.00 + PL)/-0.25 + (-)2.00 = -1.00/-2.25
It is not uncommon to achieve good centration with a spherical lens on a highly astigmatic patient. However, ordering the spherical lenses in this case could have resulted in several problems. Corneal alignment decreases rapidly as corneal astigmatism increases. A dumbbell-shaped pattern often results when horizontal bearing is present in a with-the-rule astigmat. Any areas of bearing could result in corneal flattening, followed by distortion.
A bitoric lens is an excellent option for corneas having 2.50D or greater toricity, often resulting in good centration as well as an alignment fluorescein pattern. Advancements in technology have enabled contact lens laboratories to now be more consistent in the fabrication of high quality bitoric lenses, and fitting these designs is only slightly more complicated than fitting spherical lenses. In the previous example, the final powers were determined by adding the overrefraction to the diagnostic contact lens power per meridian. Doing this not only results in a healthier fitting relationship, but also corrects the residual astigmatism, unlike the spherical design.
CASE 3: Keratoconus
J.S., a 23-year-old female, had been fit with RGP lenses three years previously after being diagnosed with keratoconus. She was experiencing a gradual onset of discomfort accompanied by reduced wearing time. Her refractive information was:
Manifest Refraction:
- OD: -4.25 - 4.75 x 157, 20/40+1
- OS: -3.00 - 2.25 x 013, 20/25-1
Keratometry:
- OD: 48.62 @ 152 / 52.12 @ 071 Mire Distortion
- OS: 45.62 @ 015 /47.25 @ 105 Slight Mire Distortion
The lenses verified with the following parameters:
| OD | OS | |
| BCR: | 7.26mm | 7.58mm |
| OAD/OZD: | 9.0/7.6mm | 9.2/7.8mm |
| Power: | -2.00D | -2.00D |
With biomicroscopy, both lenses appeared to provide good centration with approximately 1mm of movement with the blink. However, fluorescein application showed central bearing accompanied by excessive inferior edge clearance (Fig. 5). Upon lens removal, coalesced corneal staining was present (OD > OS) in the region where bearing had been observed.

FIG. 5: Central bearing and excessive inferior edge clearance on a keratoconus patient. |
J.S. was refit with the following diagnostic contact lenses:
| OD | OS | |
| BCR: | 6.49mm | 7.14mm |
| OAD/OZD: | 8.8/7.0mm | 9.0/7.6mm |
| Power: | -6.00D | -3.00D |
Both of these lenses resulted in good centration, but mild apical clearance and inadequate peripheral clearance were evident. Ultimately, the use of 6.59mm OD and 7.26mm OS base curve radii resulted in mild apical touch and a three-point touch fitting relationship (OD > OS) (Fig. 6).
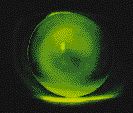
FIG. 6: Mild apical touch and threepoint fitting relationship on a keratoconus patient. |
With the appropriate overrefraction, the following final lenses were ordered:
| OD | OS | |
| BCR: | 6.59mm | 7.26mm |
| OAD/OZD: | 8.8/6.8mm | 9.0/7.4mm |
| Power: | -6.25D | -4.00D |
Although it is controversial whether harsh central bearing can result in corneal staining and scarring, it's certainly more likely that complications can occur as the relationship becomes farther away from an alignment fit.
Results from the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study have shown that selecting a base curve equal to the steep keratometry reading is a good starting point. If an apical clearance relationship is present, changing to a flatter base curve radius in 0.50D to 1.00D steps until mild apical bearing is present should help you obtain a bulls-eye or three-point-touch fitting relationship. You can enhance this fitting relationship by selecting a progressively smaller optical zone diameter as the base curve steepens. Often, this value is fairly close to the base curve radius in millimeters. For example, the relationships between optical zone diameter and base curve radius in the above case were: OD = 6.8/6.59mm; OS = 7.4/7.26mm. The use of a Burton lamp is especially advantageous for evaluating the fluorescein pattern of a keratoconic fitting relationship because its greater field of view.
Critical to Long-Term RGP Success
As these cases illustrate, fluorescein evaluation of the lens-to-cornea fitting relationship often enables you to select a contact lens that provides a more optimum, alignment fitting relationship. This minimizes the complications that could result from a fit that may compromise tear exchange or provide excessive corneal bearing. It's critical that you always remember that any contact lens design philosophy (including the philosophies of the authors) is merely a starting point. Likewise, RGP laboratories tend to vary considerably in the design parameters that they recommend (see "Setting Standards: What is a Peripheral Curve?" Schwartz et al, Contact Lens Spectrum, Oct. 1997). These factors, in combination with individual corneal topographical differences, make evaluating the fitting relationship of a rigid lens to the cornea with fluorescein critical to long-term patient success with rigid contact lenses.
Considering the large number of recommended applications -- including anyone needing critical vision, individuals with chronic soft lens-induced complications (i.e., GPC, infiltrates, coalesced staining), young people with progressive myopia, presbyopes, astigmats and irregular cornea patients -- it makes sense that any practitioner who is fitting contact lenses should be acquiring proficiency with RGPs. Proficiency is not difficult to obtain and actually requires few fits. The ability to accurately evaluate fluorescein patterns is an essential component of the proficiency process, and one that optimizes both patient and practice success with RGPs.
Dr. Bennett is an associate professor of optometry at The University of Missouri-St Louis and executive director of the RGP Lens Institute.
Dr. Johnson is on staff in the refractive surgery department and the specialty contact lens clinic at the Massachussetts Eye and Ear Infirmary, Boston.