


contact lens case reports
Identifying Dendritic Formations
BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRE, FCLSA
A 43-year-old man underwent bilateral cataract surgery in 1976 for steroid-induced lens opacities following a kidney transplant. At that time, he achieved 20/20 corrected visual acuity OU wearing Wesley Jessen aphakic, Polycon II contact lenses, which have a Dk of 12. In March of 1994, the patient's right lens broke and was replaced with an aphakic lens made of Paragon Vision Sciences' FluoroPerm 60 material, which has a Dk of 60. At a routine follow-up in February of 1998, the patient's right cornea was clear, but the left cornea had a central pseudodendritic lesion indicative of an edematous corneal formation (Fig. 1).
Historical Perspective
Edematous corneal formations are a consequence of long-term, low grade epithelial edema resulting from contact lens hypoxia. The lesions generally progress slowly and become clinically significant after six to 12 months of lens wear, but patients are often asymptomatic. Biomicroscopy examination usually reveals mild to moderate central corneal clouding, with dendritic-like linear epithelial changes. The formations rarely stain with fluorescein, as they are deep in the epithelial layer adjacent to the Bowman's layer. However, fluorescein does pool adjacent to the elevated branches of the lesion. Edematous corneal formations rarely affect vision with the contact lenses in place, but without the lenses, vision is frequently reduced secondary to corneal distortion. Historically, the incidence of ECFs was relatively high in PMMA lens wearers. Today, the advent of higher Dk RGP lenses has practically eliminated the incidence of ECFs. See Table 1 for ECF diagnostic clues.
Refitting this patient in a FluoroPerm 60 lens OS resolved the ECF lesion.

FIG. 1: Edematous corneal formation (ECF). |

FIG. 2: Contact lens solution induced pseudodendritic keratitis. |
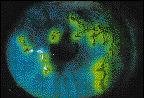
FIG. 3: Classic herpes simplex virus with fluorescein stain. |
| Lesion Location | Lesion Depth | Shape | Fluorescein Staining | |
| Edematous Corneal Formations (hypoxia) | Central | Epithelial layer | Branching, twig-like | Negative pooling around lesion (fig. 1) |
| Pseudodendritic Keratitis (chemical hypersensitivity) | Central or peripheral | Stromal/epithelium | Branching, twig-like or plaque-like | None to mild (fig. 2) |
| Herpes Simplex Virus (viral keratitis) | Central or peripheral | Stromal/epithelium | Classic branching with end bulbs | Moderate to deep (fig. 3) |
Patrick Caroline is an assistant professor of ophthalmology at the Oregon Health Sciences University and an assistant professor of optometry at Pacific University. Mark Andre is director of contact lens services at the Oregon Health Sciences University.