


CONTACT LENS COMPLICATIONS
Diagnosing and Treating Contact Lens Complications
By Carla Mack, OD
July 2000
Contact lens clinicians and researchers have put forth valiant efforts in trying to curb the number of inflammatory and infectious keratitis cases that appear to be related to contact lens wear. Educating our patients about compliance with replacement schedules, decreasing extended wear periods, using higher Dk and more bio-friendly materials have all helped to reduce contact lens corneal complications. In spite of technological advancements, many patients are still primarily motivated into compliance only after experiencing ocular complications. Taking a careful history plays a crucial role in accurately diagnosing and effectively treating noninfectious and infectious keratitis.
Diagnosing Complications
Many causes of anterior segment inflammation present much the same clinically. Differential diagnosis begins with a detailed history and the often forgotten gross external exam. The history must include contact lens brand used, advised wearing schedule versus actual wearing schedule, and the last time the contact lenses were worn and for what duration. Confirmation of overnight wear or napping in the lenses provides important clues for hypoxia. Review the cleaning regimen and current solutions, as well as the onset and course of the symptoms. Also discuss systemic health, current and past long-term medications and allergies. The gross external exam provides useful information about the patient's level of discomfort, lid swelling and redness and the pattern of conjunctival hyperemia. Biomicroscopic examination with sodium fluorescein many times simply confirms the already suspected diagnosis.
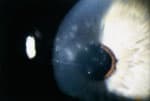
The contact lens acute red eye (CLARE) has multiple clinical manifestations. Often a history of extended wear or wearing contact lenses longer than the recommended wearing schedule is elicited. A mild inflammatory reaction presents with little more than a trace to 1+ circumlimbal injection and limbal edema with minimal comfort complaints and no visual disturbance. The cornea usually remains intact, and no anterior chamber reaction is observed. A moderate inflammatory response presents with increased patient discomfort and small reductions in visual acuity. Lid swelling, more pronounced circumlimbal injection and limbal vessel dilation are often present. Small punctate defects may be spread diffusely across the epithelial surface or found hugging the peripheral cornea. Alternatively, I have found that coalesced staining often presents in clusters of abrasion-like areas located centrally to midperipherally. An edematous cornea will appear hazy with retroillumination. Photophobia is indicative of anterior chamber involvement. The inflammatory response may produce infiltrates, a hallmark sign of the CLARE responses, which are aggregations of leukocytes released from the limbal vasculature. I see smaller infiltrates more peripherally and adjacent to dilated limbal vasculature, while larger infiltrates are found in the midperiphery. In most cases the overlying epithelium is intact.
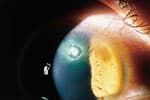
Figure 1. Ulcerative keratitis results from a damaged epithelium and tissue necrosis. |

Figure 2. Contact lens acute red eye (CLARE) has multiple clinical manifestations. |
An epithelial defect overlying a corneal infiltrate is not pathognomonic for infectious keratitis, but suspicion increases with a history of noncompliance, extended wear and moderate to severe signs and symptoms. Bacteria, whether of the normal conjunctival flora or from an external source, seek a place to thrive and replicate. Soft contact lenses coated in a nutrient-rich mucin biofilm provide a warm, moist, attractive environment to such pathogens. Normally, the ocular immune defenses such as tear film lysozymes and the multilayered web of epithelial cells are able to ward off such offenders. Any mechanical, hypoxic or immunologic trauma to the epithelial barrier allows easy access for virulent organisms to colonize and cause tissue necrosis resulting in ulcerative keratitis.
The immune response to these unwanted pathogens is a strong one. The eyelid often exhibits marked edema and the conjunctival vessels will be diffusely engorged with moderate to severe injection and a more intense circumlimbal flush. Densely packed, exposed, unmyelinated corneal nerves send disproportionate nociceptive impulses compared to the small area of necrotized edematous corneal tissue. An anterior chamber reaction compounds the discomfort experienced by the patient, and in some severe cases a hypopyon may be observed.
Ulcerative keratitis is the most severe and sight threatening complication of contact lens wear. Poggio and Schein (1989) estimated the annual incidence of ulcerative keratitis to be 4.1 per 10,000 in soft daily wear conventional lens wearers and 20.9 per 10,000 in soft extended wear conventional lens users. More recently, Cheng et al. (1999) reported incidence rates of 3.5 and 20.0 per 10,000 in daily wear and extended wear soft lens users respectively, closely matching the data of Poggio and Schein. This research indicates that no significant change in the incidence of corneal ulcers has occurred in the last decade, with the advent of disposable soft lenses or with the industry-wide acceptance of cold chemical disinfection. However, these studies did not incorporate the use of high Dk, silicone-hydrogel soft lenses in their risk evaluation of contact lens usage. In the near future, we will hopefully discover what role hypoxia plays in the development of ulcerative keratitis, but we must keep in mind that several other factors, such as bacterial adherence, tear chemistry/stability and patient compliance with recommended lens hygiene, may also play significant roles.
Management
Management of CLARE with minimal symptoms requires little more than discontinuing contact lens wear until complete resolution of all ocular signs. With moderate symptoms, I have found that patients benefit most from a combination eyedrop such as Tobradex (Alcon). In general, I prescribe the medication four times a day up to every one to two hours in more severe or symptomatic cases. If significant corneal staining is present, I avoid steroids that may hinder re-epithelialization, and prefer to use a broad-spectrum antibiotic like Polytrim (Allergan) or Tobrex (Alcon), given four times a day. I also instill one drop of Homatropine 5% in the office for those with significant pain and photophobia. Patients with minimal signs are re-examined in several days, and those with moderate to severe signs require a slit lamp exam within 24 hours to assure improvement.
Patients with Thygeson's superficial punctate
keratitis may experience RGP lens awareness.
The advent of the fluoroquinolones in the last decade has dramatically changed the management of infectious ulcerative keratitis in the ophthalmic profession. The majority of contact lens practitioners now manage most peripheral and small central ulcers in their own offices. In the past, management of these conditions was primarily in the domain of corneal specialists using fortified antibiotics, which were not readily available and were difficult to formulate. Hitting the ulcer hard early on with frequent fluoroquinolone dosage will arrest the necrotic process quickly. I advise one to two drops of Ciloxan (Alcon) or Ocuflox (Allergan) every 15 minutes for the first six hours and then every 30 minutes for the next six hours. Ciloxan ointment for overnight antibiosis and appropriate cycloplegic therapy is dosed depending on the severity of the photophobic symptoms and anterior chamber reaction. Research has indicated that adding a topical corticosteroid in addition to antibiotic therapy once the ulcer shows stabilization but is still active may enhance patient comfort and reduce scarring. Patients must be examined daily until complete re-epithelialization occurs. It has become clinically accepted that small peripheral ulcers do not require culturing, but an ulcerated area along or encroaching the visual axis, an ulcer with a diameter 2mm or greater regardless of location or a recalcitrant ulcer must be cultured. I suggest culturing with Gram stains, thioglycolate broth and chocolate and blood agar at a minimum. Many pathology labs have prepared ocular culturing kits available, which may be refrigerated for in-office use.
Differential Diagnosis: The Masqueraders
Consider several differential diagnoses when examining infectious or noninfectious keratitis in contact lens wearers. These conditions may confound the diagnosis and are frequently not related to contact lens wear at all. For example, the clinical picture of staphylococcal marginal keratitis may perfectly mimic a contact lens-related keratitis. However, the inflammatory etiology is secondary to staphylococcal exotoxins and not a direct immunologic attack against the pathogen. Signs include circumlimbal injection with peripheral infiltrates most often found in the lower half of the cornea, inferior punctate staining, neovascularization and sterile ulcerative keratitis. A history of chronic blepharitis with associated signs of red, thickened, congested lower lid margins and lash crustations are among the distinguishing characteristics that will help with this diagnosis.
The biomicroscopic corneal presentation of Thygeson's superficial punctate keratitis includes central intraepithelial infiltrates, which may produce negative fluorescein staining. The patient generally reports minimal to no discomfort, but may have contact lens awareness, especially if wearing rigid gas permeable lenses. Vision may be reduced with multiple dense opacities. Unlike contact lens-related marginal keratitis, the infiltrative lesions have a central location with no associated conjunctival or circumlimbal injection whatsoever. Thygeson's is suspected to have a viral origin.
Isolated adenoviral infections present with unilateral or bilateral conjunctival injection, superficial punctate keratitis, watery discharge and positive preauricular lymph adenopathy. Often close association with a family member or friend with a red eye can be revealed. Subepithelial infiltrates are not found for one to two weeks after the onset. They may often linger months to years after resolution of the viral conjunctivitis. A recurrent history should also alert you to a Herpes Simplex keratitis (HSK). Lid edema, conjunctival injection, pain, anterior chamber reaction, corneal SPK and infiltrates can be found in both HSK and CLARE. Differential signs for HSK may include lid vesicles, corneal dendrites with terminal end bulbs, positive preauricular lymph node (PAL) and decreased corneal sensitivity with reports of previous herpetic infection of the cornea.
The early stages of adult inclusion conjunctivitis in a young contact lens wearer are often easy to overlook. Lid edema, mild irritation, photophobia, conjunctival injection and discharge are immunologic responses common to many etiologies. Some of the more trademark signs include a positive PAL in the absence of viral sequela and a mixed papillary and follicular response concentrated on the inferior palpebral conjunctiva. The keratitis is not immediate with the limbal edema, yellowish infiltrates and pannus often occurring superiorly. A chronic nature is often uncovered with or without history of genito-urologic signs. You may find yourself being the second or third doctor the patient has sought treatment from because of lingering unresolved signs and symptoms.
Effective management and recovery of contact lens complications begins with an accurate diagnosis. Certainly, no one will discount the importance of the objective exam. However, in this world of hustle and bustle we must also remember to slow down long enough to talk with our patients and listen attentively to their history and concerns. In the end, we may still find ourselves losing the uphill battle of compliance. We continue to persevere in hopes that one day our best efforts at patient education and continued material and solution advancements will tip the scales in our favor.
Dr. Mack is a clinical assistant professor at the Ohio State University College of Optometry. She is also chief of optometry at the Wilce Student Health Service at OSU.
| Pseudomonas aeruginosa | Gram |
| Haemophilis influenza | Gram |
| Serratia marcesans | Gram |
| Neisseria gonorrhea | Gram |
| Staphylococcus aureus | Gram + |
| Staphylococcus epidermis | Gram + |
| Streptococcus viridans | Gram + |
| Streptococcus pneumoniae | Gram + |
TABLE 2: Clinical Signs of the Red Eye
| CONJUNCTIVA INJECTION | CORNEAL INFILTRATES | PREAURICULAR NODES | CELLS AND FLARE | ETIOLOGY | |
| CLARE | Circumlimbal | Peripheral | - | -/+ | Inflammatory |
| Ulcerative Keratitis | Diffuse | Peripheral/Central | - | + | Bacterial, Fungal, Protozoal |
| Marginal Keratitis | Circumlimbal | Peripheral | - | - | Inflammatory |
| Thygesons | None | Central | - | - | Viral |
| Adenoviral | Diffuse | Central | + | - | Viral |
| HSK | Diffuse | Central | + | -/+ | Viral |
| Inclusion Conjunctivitis | Diffuse | Peripheral | - | - | Parsitic |