


contact lens case reports
Diagnosing and Managing Pellucid Marginal Degeneration
BY PATRICK J. CAROLINE,
FAAO, & MARK P. ANDRÉ, FAAO
November 2000
Patient D.W., a 31-year-old male, presented with decreased visual acuity with his habitual spherical soft lenses. At initial examination, his distance VAs were OD 20/20 and OS 20/40. The manifest refraction was OD 6.25 sph. 20/20 and OS 3.50 2.25 x 083 20/25. Keratometric readings were OD 44.87 @ 180 / 45.12 @ 90 and OS 43.50 @ 80 / 46.50 @ 170. Slit lamp examination revealed inferior corneal thinning OS approximately 1 mm from the limbus, indicative of pellucid marginal degeneration (PMD) (Figure 1). We noted no corneal thinning OD. Videokeratography OS showed marked corneal steepening at 4 o'clock and 8 o'clock, resulting in a typical "butterfly wing" pattern (Figure 2), essentially diagnostic of PMD. The right eye showed no topographical signs of PMD.

Figure 1. Inferior corneal thinning characteristic of PMD. |
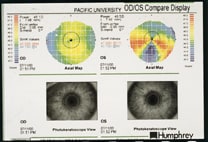
Figure 2. Patient's corneal mapping illustrating the unilateral PMD. |
Defining PMD
PMD is a bilateral corneal disorder hallmarked by inferior stromal thinning, resulting in high degrees of against-the-rule corneal astigmatism. It affects both genders, most often between the ages of 20 and 40, with no apparent hereditary transmission. It is characterized by a narrow band of corneal thinning 1 to 2 mm in width located in the 4 o'clock to 8 o'clock position. There is a 1 to 2 mm wide region of uninvolved "normal" cornea between the thinned region and the inferior limbus. The inferior cornea is free of vascularization or lipid infiltration, differentiating PMD from other peripheral thinning disorders such as Terrien's marginal degeneration and Mooren's ulceration. It is differentiated from keratoconus in that with PMD, central corneas retain normal thickness.
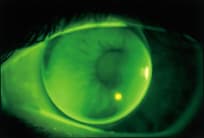
Figure 3. An "on K" spherical RGP lens fitted on the patient's left
eye.
Management of PMD
Spectacle correction is often satisfactory in the early stages of PMD due to the minimal degree of induced irregular astigmatism. However, in more advanced cases when contact lenses may be indicated, the fitting is often complicated by high against-the-rule astigmatism (Figure 3). Historically, PMD has been best managed with aspheric RGP designs, often with a piggyback soft lens.
We successfully managed this rare case of unilateral PMD with a spherical RGP lens OD and a bitoric lens OS (Figure 4).
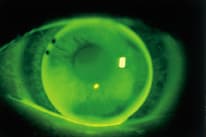
Figure 4. The final bitoric lens fitted on the patient's left eye.
Patrick Caroline is an associate professor of optometry at Pacific University and an assistant professor of ophthalmology at the Oregon Health Sciences University.
Mark André is director of contact lens services at the Oregon Health Sciences University.