


Making RGP Fitting Efficient and Successful
Robert Davis, OD,
FAAO; Patricia Keech, OD, FAAO; Burt Dubow, OD; & Keith Ames, OD
October 2000
Fitting RGPs can be as efficient and satisfying for both patient and practitioner as fitting soft contact lenses.
In today's high energy, hurried society, practitioners must prescribe and fit contact lenses as quickly and efficiently as possible. However, this should not be accomplished with any compromise in vision or eye health. Rigid gas permeable (RGP) lenses should be a valuable part of a practitioner's armamentarium when fitting contact lenses. For RGPs to become a vital part of a contact lens practice, the initial experience has to be satisfying to the patient and efficient for the practitioner.
The Right Mood
Patient excitement for contact lens wear is created when the first lens placed on the eye performs optimally with minimal sensation. We must optimize our opportunities to create a positive experience with our contact lens patients. RGP lenses, soft lenses and refractive surgery are all competing for the same ametropic patients. This competition places pressure on the various correcting modalities prescribed by practitioners. The diagnostic correcting experience must result in a positive outcome for the patient to achieve success.
Avoid biasing the lens selection. Each modality has its own benefits and risks. Inform the patient that lens modality is not as important as a successful fit and comfortable, safe and effective contact lens wear. Both patient and practitioner are partners in the fitting process, and every effort will be made to achieve a successful fit.
RGPs, in particular, need to be presented with confidence. The benefits of good vision, eye health, ease of handling, durability and possible slowing down of myopic progression in young people are some advantages of RGP lenses. Certainly the initially greater lid awareness needs to be mentioned as well. Mention to the patient that RGP fitting is a process, and that we need to take it one step at a time. If a diagnostic fitting is performed, patients can obtain a reasonable idea of the quality of vision and exactly how challenging the first few days are. When communicated in this manner, most patients, including previous soft lens wearers, are pleasantly surprised at the results. Patients can be told that the initial experience is the most difficult, and most of the adaptation occurs during the first few days. A good phrase to use is that RGPs keep getting better every day, while the opposite may be true with soft lenses.
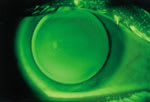
An apical alignment fluorescein pattern |

A well centered RGP lens |
Diagnostic or Empirical Fitting?
Perhaps the biggest controversy in fitting RGP lenses efficiently is whether to continue using diagnostic lenses or simply to either provide an empirical design to the laboratory or have the laboratory design the lenses based upon refractive and/or topographical information. In fact, if contact lens practitioners were polled nationwide, a strong argument could be made for both approaches. Two authors use diagnostic lenses on all RGP patients, while two typically fit lenses empirically. Obviously both approaches can be quite successful. However, for diagnostic fitting to be performed in an efficient manner, the fitting process should be made as satisfying to the patient as possible. For empirical approach success, the specific RGP lens should be both well designed and manufactured.
Diagnostic Fitting
Diagnostic fitting allows the patient to experience lens wear immediately, getting them "over the hump" with initial expectations and anxieties. It also provides the contact lens practitioner with the opportunity to evaluate all the variable fitting factors, including the lens-to-cornea fitting relationship and make any desired changes to improve the fit. The patient often leaves the office with the perception that future success will be achieved. If a poor fitting relationship or patient dissatisfaction results, different options can be attempted before the patient leaves the office. In addition, contact lens practitioners need to make many observations beyond lens diameter and base curve radius. Such factors as lid tension, pupil size, tear flow, movement, lateral centration, peripheral curve relationship, lens movement, lens position and wetting characteristics of the lens material need to be evaluated to achieve an optimal fit.
Obviously when diagnostically fitting RGPs, the process has to simulate the efficiency of fitting soft lenses. Soft lenses have pushed the envelope with instant patient gratification after the diagnostic fitting process. RGPs must match this experience. This process begins with initial comfort. Using a topical anesthetic, although not advocated by every practitioner, will greatly reduce any initial apprehension and make the first few minutes of lens wear quite acceptable. The anesthetic will then wear off and the patient will gradually experience lens sensation. Anesthetic use also allows the practitioner to quickly assess the lens-to-cornea fitting relationship as opposed to waiting as long as 20 to 60 minutes for the initial reflex tearing associated with a foreign body sensation to subside.
A sufficient RGP contact lens inventory helps you and the patient succeed with diagnostic fitting. Vision is associated with initial comfort in most patients' minds. If the initial diagnostic lens provides good visual acuity, clear vision is a great motivating factor in making the lenses seem as though they are more comfortable. This also results in fewer patient questions about the lens fitting relationship and vision. Keeping a gas permeable lens inventory also provides patients with a service when a lens is lost or needs to be replaced. Many successful RGP wearers have felt they had no choice but to change to soft lenses when a replacement RGP was not available, and they had no desire to wear spectacles, even temporarily. Having replacement lenses in the office can eliminate this inconvenience.
Empirical Fitting
Empirical fitting has gained greater acceptance and success in recent years. Empirical fitting is time-efficient and also quite accurate because the fitting is assessed after adaptation, which allows the lens mechanics to stabilize. Although a higher reorder rate may be present, for practitioners without an inventory this system makes sense as the first lens the patient wears should approximate, if not equal, the indicated prescription. Good vision is immediately achieved. Avoid using a 3.00D diagnostic lens on all myopic patients for this reason. Unless patients' correction equals the diagnostic lens power, they will notice the reduced visual acuity, and this can affect their perception of RGP lenses. The power and fitting relationship can be fine-tuned, if necessary, at the one-week follow-up visit.
Successful empirical fitting has been achieved with greater success due to the introduction of numerous lens designs with standard parameters (aspheric peripheries, set diameters, ultrathin construction). This is made possible by the higher quality of manufacturing methods in use today. In addition, corneal topography with design software can result in good first-fit success when empirically ordering the lenses. Empirical fitting should be attempted only after experience has been gained with diagnostic lenses. Therefore, a good understanding of lens design and evaluation is gained which can then be applied to the empirical order. Likewise, the authors all believe that diagnostic lens application is important when fitting specialty lens designs, notably many bifocal, keratoconic and orthokeratology designs.
Comfortable Lens Design
To make RGPs efficient and ultimately successful, the lens design must be as comfortable as possible. As a result of higher quality manufacturing, modern edge designs are more consistently smooth and comfortable. Nevertheless, inspect the edge prior to dispensing the lens. In addition, the ultrathin designs today allow for greater likelihood of achieving a lid attachment fitting relationship as a result of less overall mass. Consider several other factors as well, including lid position, palpebral aperture size and patient sensitivity. For patients with normal-to-small aperture sizes, a lid attachment fitting relationship can typically be obtained with standard diameters (9.2mm to 9.8mm). A smaller overall diameter (8.5mm to 9.0mm), fit slightly steeper, achieves an intrapalpebral fitting relationship in patients with steeper than average corneal curvatures and/or a large palpebral fissure size. Patients who are especially sensitive to contact lens wear may benefit from a larger diameter lens which tends to move less on the eye and results in less initial awareness.
Successfully Manage Adaptation
Remain realistic but encouraging when discussing the adaptation process with patients. Tell them to give their lenses, at minimum, one month before they pass final judgment on the comfort of their lenses. It is not uncommon for a patient who is experiencing some difficulty at two weeks to be totally satisfied at four weeks. They should increase their wearing time every day and, in doing so, the normal adaptive symptoms (awareness, light sensitivity, itching) should go away.
For patients who exhibit mild lens awareness, all-day wear can happen sooner, sometimes in as little as four days. Let them know the nature of perceptual adaptation. RGP lenses do not induce more initial awareness than soft lenses because they are rigid; they are felt more initially because they are smaller and move more with the blink.
RGP Fitting Pearls
Efficient and successful RGP contact lens fitting has been made possible as a result of better quality, reproducibility, faster delivery time and availability of inventories by contact lens manufacturers. In addition, using trained staff members for lens verification, lens application and patient education is essential. Patients must feel competent in lens handling prior to leaving the office. It is not uncommon for a patient to fail due to handling problems during adaptation. If the staff member feels confident in the presentation, the patient will benefit. In addition, ask patients about their lens handling at the one-week visit. Any problems they mention can be rectified at that time.
Likewise, another time saver is the use of +/ 0.50D and 1.00D flipper bars for overrefraction. If the lens you requested is close to the final parameters, and the patient sees 20/20, place the +0.50D lenses on the flipper bar in front of the patient's eyes and ask if his vision blurs. If it does, and the 0.50D lens does not improve vision, you have a quick overrefraction confirming that the power is correct (See Efficient Fitting Guidelines, Page 44).
RGP fitting can and should be efficient and successful. In the competitive environment in which we practice today, RGPs can create our most enjoyable and successful patients while helping to make the practice of optometry more rewarding and profitable.
Dr. Davis is developing an eyecare specialists practice outside of Chicago and is serving as Past Chair of the Contact Lens Section of the American Optometric Association.
Dr. Keech is in private practice in Shoreline, Wash., and has served as a faculty member at Indiana University and as clinic chief at Group Health Cooperative of Puget Sound.
Dr. Dubow is in private practice in St. Cloud, Minn., and a past chair of the AOA Contact Lens Section.
Dr. Ames is in private practice in Chilicothe, Ohio, and a technical and marketing consultant to the contact lens industry.
Efficient Fitting Guidelines1. Be positive in the presentation. 2. Use a topical anesthetic with apprehensive patients. 3. If diagnostic fitting, using a fitting inventory optimizes the initial visual experience. 4. Empirical fitting has the benefit of providing optimum vision during the initial lens application process. 5. Smooth edge and ultrathin designs can increase initial comfort. 6. Consider factors such as lid profile and patient sensitivity when selecting the lens diameter; a larger diameter typically moves less and results in less awareness. 7. Advise patients to give RGPs, at minimum, one month to feel comfortable. 8. Have competent, confident staff members who will ensure that patients feel confident in handling lenses; use the one-week follow-up visit to confirm this. 9. Flipper bars are a quick and efficient means to confirm whether a power change is indicated. |