


MULTIFOCAL LENSES VS MONOVISION
Comparison of Multifocal Lens Performance to Monovision
By Susan J.
Gromacki, OD, MS, FAAO, and Eric Nilsen, OD
May 2001
This study surveyed patients to determine if multifocal contact lens wearers are as satisfied with their lenses as monovision wearers.
With the advent of new designs and materials, eyecare providers are prescribing multifocal contact lenses more than ever. Monovision, however, remains practitioners' first choice for contact lens-wearing presbyopes for ease of fit, lower patient expenses and higher patient satisfaction as compared with multifocal contact lenses.
The purpose of this study was to determine whether presbyopic patients wearing multifocal contact lenses were as satisfied with the performance of their lenses as those utilizing monovision.
Study Methods
Some 113 patients returned questionnaires distributed to contact lens wearers of the New England Eye Institute. The surveys were anonymous and self-administered. They assessed clarity of distance vision, clarity of near vision, comfort, lens handling and overall satisfaction.
The survey rating scale ranged from 1 (poor) to 10 (excellent) in increments of one unit. Each of the 10 possible answers was assigned an exact descriptor. For example: 1) My lenses are extremely uncomfortable from the moment I put them on. I cannot wear them at all; and 10) My lenses are exceptionally comfortable. I have no discomfort problems and am happy wearing them all day.
The surveys questioned three categories of contact lens patients: monovision wearers, multifocal contact lenses wearers and a control group of soft spherical lens wearers. All three groups contained both full- and part-time lens wearers. The monovision group (n=29) consisted of experienced contact lens wearers in either rigid or soft materials. The multifocal group (n=33) contained 24 new (one month of multifocal lens wear) Sunsoft Multifocal soft contact lens wearers and nine experienced rigid and soft multifocal lens wearers. The control group had 51 members.
Results
Table 1 summarizes the mean responses for the monovision versus multifocal patients for distance vision, near vision, comfort, handling and overall performance. There were no statistically significant differences for any of these indices between the two groups (p values = 0.73, 0.43, 0.71, 0.54 and 0.51). There were no differences between the two sub-groups of multifocal contact lens wearers or between either sub-group and monovision wearers. We found no significant differences within any category between presbyopic and non-presbyopic patients, except for near vision with the soft multifocal lenses (7.2 ±2.1, p=.0001) (Figure 1).
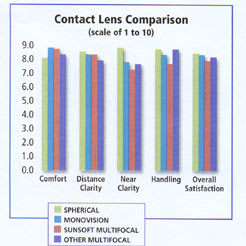
Figure 1. Survey results
Discussion
This study found slightly better overall patient satisfaction in spherical lens wearers as compared with monovision or multifocal contact lens wearers. In addition, this study found no statistically significant differences between the two latter modalities. Many factors can influence success with monovision: ocular dominance and sighting preference, interocular suppression of blur, age, reduced stereopsis and reduced contrast sensitivity. Similarly, success with multifocal lenses has been limited by inadequate vision at distance or near, reduced contrast sensitivity, increased chair time, practitioner inexperience in fitting the lenses, limited lens designs, expensive products, poor lens reproducibility and variations in both pupil size and eyelid factors. Today's multifocal contact lens technology, however, is better than ever. Sources report success rates of 60 to 70 percent or more.
Other surveys have found similar results to this one. A survey comparing monovision with the Ocular Sciences, Inc. Hydron Echelon diffractive bifocal contact lens found no subjective differences in distance vision, intermediate vision, vision in dim light, night driving, overall acceptance or comfort, although monovision was subjectively preferred for near vision. Also, participants in a study by Situ et al rated their vision in the Vistakon Acuvue Bifocal contact lens better than with monovision for distance vision in good and poor lighting and near vision in good lighting. They assessed their near vision in poor lighting to be better with monovision.
Monovision remains a more popular choice than multifocal contact lenses for correcting presbyopia. This modality has higher reported success rates, generally between 60 and 80 percent. For example, Back, Holden and Hine found a 67 percent success rate (after three months of lens wear) with monovision, 42 percent with a concentric center-near bifocal design, and 37 percent with one eye concentric center-distance and the other eye concentric center-near. Other factors include ease of fit, especially of patients with astigmatism, and lower patient costs. Even so, some studies have found a majority of patients to prefer bifocal contact lenses to monovision.
Perhaps one reason why our study found almost equal survey results for multifocal contact lenses and monovision was that most of the multifocal subjects were wearing the same lens (Sunsoft Multifocal) fitted by the same practitioner (SG). In addition, the patients were self-selected from a newspaper advertisement. Gussler et al state that two factors are essential for success with multifocal contact lenses: patient motivation and proper fitting. Both elements were present in this case.
|
TABLE 1: Monovision vs. Multifocals |
||
|
Patient Responses (Out of 10) |
||
| Monovision | Multifocals | |
| Distance vision | 8.3 ±1.5 | 8.2 ±1.5 |
| Near vision | 7.8 ±1.9 | 7.3 ±2.4 |
| Comfort | 8.8 ±1.5 | 8.6 ±1.3 |
| Handling | 8.3 ±2.0 | 7.9 ±2.1 |
| Overall | 8.3 ±2.3 | 7.9 ±1.9 |
The Sunsoft patients were also subjected to a prescreening process that required all patients to be free of ocular disease, have ¾0.75D of spectacle cylinder and a best-corrected vision of at least 20/20 in each eye at distance and near. The monovision patients and the other bifocal patients were randomly selected from the practice database.
One other notable point concerns the Sunsoft wearers in the study. A year later, seven out of the 21 patients that we were able to contact were still wearing the Sunsoft lenses (Nine out of 21, or 43 percent, were wearing any brand of multifocal contact lenses). One may assume that if only experienced multifocal wearers were surveyed, the average numerical responses for the multifocal group would have been higher. We can assume that the successful Sunsoft wearers' responses would be the same at one month as at a longer time period. Bierly et al surveyed Dist-O-Con, Inc.'s Solitiare Bifocal lens wearers for distance and near vision (night and day), glare, comfort and overall satisfaction at both one and six months of wear and found few differences in responses.
Another reason the bifocal wearers' responses in our study are more positive than in previous studies is the predominance of a newer design, the Sunsoft Multifocal, in the response group. The lens was introduced in 1996, after many of the aforementioned studies were completed. Sunsoft has since discontinued this lens and replaced it with the Additions planned replacement multifocal.
Our study found that both new and experienced multifocal contact lens wearers statistically were as satisfied with their lenses as were monovision patients.
The authors thank Scott Lathrop for his statistical assistance and Kim Lefevre, OD, for her help with data collection.
To receive references via fax, call (800) 239-4684 and request document #71. (Have a fax number ready.)


|
Multifocal Contact Lens Fitting Tips |
|
|
|