


Multifocal Contact Lens Update
DOUGLAS P. BENOIT, OD, FAAO
November 2001
Modern manufacturing makes old designs more functional for the maturing population.
We have seen many changes in multifocal contact lenses over the past five years. Some progressive practitioners and manufacturers have realized the growth potential with the aging population, but few of us imagined that reproducible, disposable multifocals would be a reality or that there would be such an explosion of new presbyopic options. Still, many practitioners avoid bifocal/multifocal contact lenses, especially rigid gas permeable (RGP) lenses, due to negative prior experiences or a fear of failure with a complex design. Knowledge of the design basics and a systematic approach can breed success.
Demographics
Few patients realize that bifocal/multifocal contact lenses have been available for over 50 years. Even some practitioners are unaware of it. Word is spreading, however, and you need to be ready to assist presbyopes in your practice.
Between four and five million people turn 40 each year, and there are now over 100 million presbyopes. The baby boom generation has increased the 40- to 55-year-old age group in every market. This is most apparent in the healthcare field. Health clubs are seeing huge increases in memberships, and anything that can make people feel younger and appear more youthful is enjoying great success.
Your aging patients do not want to compromise their lifestyles just because they now need reading or multifocal correction. They want the vision flexibility they had at 30. Many present single vision contact lens wearers fear that they must give up contact lenses in order to keep good distance and near vision. This is an opportunity for you to simultaneously educate patients and grow your practice.
Screening
You need to have rational criteria for screening potential multifocal candidates. First, assess the patient's motivation to ascertain whether he will comply with the visits and lens changes necessary for success. Then, discuss your patient's expectations. If he demands perfect vision at all distances and at all times, he will most likely end up dissatisfied. Make sure the patient realizes that presbyopia requires compromise. There are times when neither contact lenses nor eyeglasses are perfect.
You should also consider the patient's ocular health and physiology. If the eye and adnexa are not appropriate, the patient will not do well. The patient needs a healthy cornea and conjunctiva, good lid structure and function and a wet enough eye to sustain a contact lens. Age affects all of these areas, so it is important to be critical. If a patient is unlikely to succeed, inform him directly.
If ocular health and physiology are satisfactory, then discuss your patient's vision requirements at work and play. People who need very sharp vision at any or all distances may be disappointed, as may those who work in low light. Most patients have some computer use in their day, which necessitates reasonable intermediate distances vision. Consider the patient's refractive error. In the past, we believed that patients with less than 1.00D of distance prescription with too high an add power would not do well. While both of these types of refractive error are more challenging, today's lenses better meet that challenge.
Options
Discuss with your patients the various presbyopic vision correction options. For some patients, eyeglasses or refractive surgery may be most appropriate. For those patients for whom contact lenses are the best choice, present the different approaches available. For outdoor enthusiasts, using distance contact lenses with reading glasses is often a good compromise, while office workers may prefer near/intermediate range contact lenses with an over-refraction for distance in spectacles. The majority of patients, however, really desire a contact lens-only approach.
In the past, monovision was the method of choice for early and middle presbyopes. This can give good vision at various distances, and it is less time-consuming and less expensive for both patients and practitioners than bifocals. Monovision does often disturb depth perception, especially as the bifocal add power increases. Bifocal or multifocal contact lenses can eliminate some of this difficulty, and they allow a more equal image size and quality between the two eyes and can cover a broader range of prescription needs. Monovision and bifocal/multifocal contact lenses are not mutually exclusive but rather complementary approaches.
Practitioners' attitudes are changing, as shown by surveys in 1998 and 2001 of some Diplomates of the Section on Cornea and Contact Lenses of The American Academy of Optometry. Although such surveys do not have scientific accuracy, they do indicate directions and trends. The respondents estimated the modality they used for early presbyopes in the categories of discontinue contact lenses, near Rx over contact lenses, monovision contact lenses, modified monovision (one bifocal and one single vision), bifocal soft contact lenses, bifocal RGP contact lenses and others. From 1998 to 2001, there has been a reduction of monovision, although it is still quite popular, and an increase of RGP and soft bifocals/multifocals. Because of significant advances with bifocal/multifocal contact lenses, practitioners' attitudes have changed.
|
|
|
|
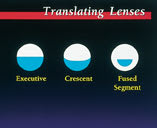
Figure 1. Various segment configurations of translating/alternating vision bifocal contact
lenses |
|
General Designs
The two basic bifocal/multifocal design concepts are translating, or alternating, image and simultaneous image. With the alternating image design lenses, the top of the lens usually has the distance vision area and there is "a line" at which point the near vision area is engaged. This is an easy concept to explain to the patient because bifocal eyeglasses work the same way and is what patients visualize when we discuss bifocal contact lenses (Figure 1).
Theoretically, in straight ahead gaze, patients see well at distance and when patients look down, the lens translates so the near correction covers the visual axis. When the contact lens is on the eye, with some special designs, the image "jump" phenomenon experienced with many eyeglasses is eliminated when moving from one zone to the other. For some patients this can actually make the translating bifocal contact lens easier to adjust to than bifocal eyeglasses. However, patients generally lose intermediate-distance focus with translating bifocal contact lenses. Translating designs are currently available only in RGP materials.
|
|
|
|
Figure 2. Schematic of a concentric
bifocal contact lens with a central
distance zone and the annular near zone in blue. |

With the simultaneous image design, theoretically the retina receives input from multiple distances at the same time with different clarity of the images. The visual system and brain must determine which image is most important and adjust to give good vision at a particular distance. Some translation may occur, and many of the newer rigid lenses rely on this to enhance the image at all distances. Simultaneous image design multifocal lenses can be concentric, aspheric or diffractive. Simultaneous image designs are available in soft or rigid materials.
With a concentric design, a central zone of distance or near power focus is surrounded by one or more rings that contain the opposite power (Figure 2). Some even alternate distance and near in a repeating pattern which helps to improve pupil coverage and visual input with variations of illumination and pupil size. The widely used Acuvue Bifocal (Vistakon) is the prime example of this.
|
|
|
|
Figure 3. Center-distance back surface aspherics have increase of plus or
decrease of minus power from center to periphery. Center-near front surface aspherics have decrease of plus or increase of minus from center to periphery. |
|

Aspheric designs use an aspheric front or back surface to create the multifocal effect (Figure 3). As a rule, front surface aspheric designs are center-near and back surface aspherics are center-distance. Each type has its own merits, as center-near designs tend to favor near and intermediate vision, while center-distance lenses usually give better distance focus. Which one to choose depends on the patient's individual needs and ocular characteristics (Figure 3).
With diffractive design (Figure 4), light entering the eye is diffracted to produce the images the retina receives (Figure 5). The diffractive design has a distance center and a series of diffractive phase-plates that surround it. As the add power increases, the number of phase-plates increases, and they get closer together (Figures 4 and 5).
|
|
|
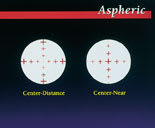

Figure 4. Diffractive design with a series of phase-plates (echelettes).
Figure 5. Top illustrates refraction while bottom shows diffraction of light.
RGP Bifocal/Multifocal Lenses
Translating The Tangent Streak (Fused Kontacts) looks like an executive spectacle bifocal with a segment that is flat on top and runs from edge to edge. Segment height and power can be varied and a truncation and prism ballast can be ordered. The Metro-Seg (Metro Optics) is a crescent-shaped bifocal design which offers unlimited add power and more stable rotation properties. The Presbylite RGP multifocal (Lens Dynamics) has a "sectored design" with a wedge-shaped segment that has an aspheric intermediate zone at the top. Prism ballast adds to +3.00D are available. The FluoroPerm ST (Paragon) utilizes an encapsulated segment made from a different material than the rest of the lens. The lens looks like a straight-top spectacle lens blank, can have both the segment height and power varied and incorporates truncation and prism ballast for stabilization. Although some labs may still inventory Fluoroperm ST buttons, in the future the lens will not be available.
|
|
|
|
Figure 6. A translating DeCarle design RGP
bifocal. |
|

An older but still useful design is the decentered DeCarle (Figure 6). With its small distance segment that is located slightly above lens geometric center and a surrounding lens that provides the near power and the fitting relationship, the lens can usually be made thinner than other translating designs and boasts unlimited add powers with available prism ballast and truncation. Many of the smaller local contact lens laboratories can produce such a lens.
West Australian company Gelflex Laboratories has recently received FDA approval for its new Triton Translating Bifocal Soft Contact Lens. The design of the Triton lens allows for the incorporation of a patient's full prescription, including toric powers.
Simultaneous Vision Many simultaneous image RGP bifocals are available. One unique design is the Zebra bifocal (Breger Vision). It is a concentric design that has a distance center with alternating near and distance rings covering the rest of the lens. Like many simultaneous designs, it must center well in primary gaze to work properly.
Aspheric designs Aspheric designs make up the bulk of the RGP simultaneous image design category. Earlier generations of these lenses had very steep base curves-to-cornea fitting relationships and high eccentricity values. Newer versions generate the same near power with lower e-values and more normal fitting relationships, such as the Essential RGP lens (Blanchard Contact Lens) and the UltraVue 2000 GP lens (Opti-Centre Laboratories). Both are fit very much like a conventional single vision RGP with an alignment fitting philosophy (Figure 7). These lenses need to translate up on downgaze to take advantage of the near power found in this mid-periphery. The UltraVue 2000 GP is available as either center-distance or center-near. It is frequently fit with a center-distance lens on the dominant eye and a center-near lens on the non-dominant eye in a modified monovision approach. The Essential RGP has multiple lens diameters and three add ranges (Figure 8). There are many more aspheric design, simultaneous image lenses available today. Local laboratories are a good source for manufacturing lenses that work well and for providing consultation advice on multifocal fitting.

|
|
Figure 7. Aspheric RGP multifocal with superior positioning and good base curve-to-cornea relationships.
Figure 8. The Essential RGP multifocal.
Soft Bifocals/Multifocal Lenses
Diffractive The Echelon (Ocular Sciences) is the only diffractive lens available. As it works via phase-plate optics to diffract rather that refract the images, it is a nearly pupil-independent design which has three add powers but only one base curve and diameter.
Concentric There are a few concentric designs in existence. One of the oldest concentric designs is the Bi-Soft (now LL-Bifocal from Lombart) (Figure 9). It has a center distance with a near periphery, multiple base curves and add powers to +3.00D. The Simulvue (Unilens) is another concentric design, but it has a center-near design (Figure 10) with adds to +3.00D and two segment sizes. A +3.50D add is also available in limited other parameters.

|
|
| Figure 9. Schematic of a concentric center-distance soft bifocal contact lens. |
Figure 10. Schematic of a concentric center-near soft bifocal contact lens.
Like translating RGP lenses, concentric and diffractive soft lens designs tend to be lacking at the intermediate vision level. Modified monovision can help, and the experienced fitter adapts these lenses to the patient's needs.
|
|
|
|
Figure 11. The Acuvue Bifocal provides alternating distance and near
zones. |
|
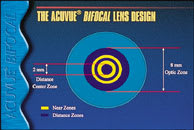
The most significant new concentric design is the previously-mentioned Acuvue Bifocal. Instead of the conventional two-zone concentric design, this lens is multi-zone with five alternating distance and near zones, starting with distance power in the center (Figure 11). The multi-zone design better provides distance and near power coverage of the pupil as it dilates or constricts with contact lens movement. Add powers are available from +1.00D to +2.50D in 0.50D increments, and it is a bi-weekly planned replacement modality.
Aspheric Though aspheric soft designs do provide intermediate vision, it is sometimes necessary to use a modified monovision approach for maximum acuity. As with RGP aspherics, soft aspherics may have a center-distance or a center-near design. While RGP aspherics are usually center-distance designs, soft aspherics are mostly center-near.
Center-distance soft aspherics include the V/X (Aero Contact Lens), which is available in two base curves and two lens diameters with adds to +3.00D. Like most soft bifocal/multifocal lenses, centration is essential to good vision. Specialty Progressive (Specialty Ultravision) is a planned replacement, center-distance aspheric design. It has two base curves and an effective add of +3.00D with a modified monovision fitting approach.
Center-near aspheric designs include Softsite (Unilens). It offers two base curves, front aspheric adds to +2.50D and is lathe cut. The Additions (Sunsoft) multifocal has three add ranges, one each for low, medium and high power requirements. This front surface, aspheric, center-near design is replaced quarterly. Quattro (Blanchard) is a quarterly replacement aspheric lens, with a center-near configuration and fitted using the modified monovision philosophy. Focus Progressive (CIBA Vision) is a center-near aspheric with a two-week to one-month replacement schedule. It is approved for both daily wear or extended wear for up to one week. CIBA Vision recently unveiled Focus Dailies Progressive which, as the name implies, is discarded daily. The parameters are +5.00D to 6.00D in the same 69 percent water nelifocon A material as the original Focus Dailies. However, it is available only in the 8.6mm base curve.
The UltraVue 2000 4-cycle (Opti-Centre Laboratories) lens has a center-distance design (for the dominant eye) and a center-near design (for the non-dominant eye). The new CooperVision Frequency 55 Multifocal has a similar design.
Soft Toric, Bifocal/Multifocal Designs
These lenses are available as concentric or aspheric designs with center-near or center-distance configurations. UCL Multifocal Toric (United Contact Lens) has an aspheric back surface which generates a center-distance design. The front surface contains the cylinder power to correct astigmatism up to 3.00D. The Horizon 55 BiCon Toric (Westcon Contact Lens) is a concentric center-near lens that can correct up to 5.00D of astigmatism and +3.00D of add. Essential Soft Toric Multifocal (Blanchard Contact Lens) has a front aspheric, center-near design with posterior toricity and anterior double slab-off for stability. Using a slight modified monovision fit, effective adds to +2.75D can be achieved. The UltraVue 2000 Multifocal Progressive Toric (Opti-Centre Laboratories) is available with a center-distance design and a center-near design for the dominant and non-dominant eyes, respectively, with adds to +3.50D. It utilizes modified monovision.
Fitting Approaches
How you handle patients who need bifocal/multifocal correction can have a dramatic effect on your practice. First and foremost, patients must realize that presbyopia is a compromise. Once a patient is at the point where a single vision lens is no longer adequate for all viewing tasks, compromises must be made to see comfortably throughout the day. Patients will either remove their glasses to read, put on their glasses to read or have difficulty seeing at some distances. Their eyes no longer perform as they did at age 30. This needs to be stressed to your patients. If they cannot accept this fact, they are probably not good candidates for multifocal contact lenses.
For those patients who clear this hurdle, formulate a plan for satisfying their vision needs. There are many methods for achieving their goals. With the total bifocal fit, each eye gets the maximum vision for distance and for near. Ideally this is the best approach, but in reality it can create visual stress because the visual system has a dominant eye, and this dominance needs to be respected. The dominant eye can be determined by methods such as the simple "hole in the hand" test or fogging techniques where plus power over-correction is added to each eye in turn, and the eye that accepts the most plus is considered the non-dominant one.
Modified monovision is a good way to solve the dominance issue when the dominant eye is given the better correction for distance and the non-dominant eye is given a slightly greater add power. In this way both eyes have nearly equal visual input, and patients adapt easier. Many manufacturers have long recognized this and reflect it in their designs and fitting nomograms to simplify and enhance fitting success and to reduce chair time. Even a so-called total bifocal fit usually results in a form of modified monovision.
Do not hesitate to fit bifocal or multifocal contact lenses because of a fear of failure with more complex designs or negative prior experiences. Neither of these factors should be an obstacle any longer. Today's design and parameter availability and the very generous exchange or cancellation policies of most laboratories allow multifocal fitting with zero material outlay and risk. If the fit is discontinued, the lenses can be returned and a credit issued. You must decide what, or even if, to charge the patient for professional fees in this situation.
Patient Movitivation Many patient and practitioner factors bear on success rates. As mentioned, patient factors include motivation, goals and ocular health. The patient's motivation to wear bifocal/multifocal contact lenses is of primary importance, and it allows the patient to physically, mentally and visually move through the initial period of adaptation. It is not uncommon to need at least three or four follow-up visits to fine-tune vision and other wearing issues. You need to assure patients that this is a normal facet to multifocal contact lens wear. If they think one visit will result in perfect vision at all distances, they will fail.
A patient's goals and expectations for contact lens use must be realistic. Be up-front with patients as to what today's lenses can and cannot do. Use the 80/20 analogy, i.e. the patient can expect that the bifocal/multifocal contact lenses will perform as desired about 80 percent of the time, but 20 percent of the time he will need something else to get the visual result he seeks. This may involve a pair of reading eyeglasses to enhance very fine or close objects, reverting to his regular eyeglasses, etc. As long as the patient knows what to expect, he will adjust.
Be sure that the patient's external ocular health is sound. Resolve issues with the lids and/or the accessory lacrimal glands before the fit. The cornea and conjunctiva must be clear and quiet to ensure a successful physiological result. Ocular surface dryness is probably the single biggest problem seen in the presbyopic patient, and the cause of the dryness should be assessed and remedied before the contact lens trial begins. Warm compresses, ocular lubricants or punctal plugs may be the solution.
Practitioner Motivation Practitioner motivation is as important as patient motivation. If you are excited and believe it can be successful, you enhance your motivation and approach to your patients. Develop adequate experience with some of the various designs. You do not need expertise with every bifocal/multifocal contact lens design, but you should master and have available inventories of the three or four different lenses, in both soft and RGP materials, that you use regularly. You will know the pros and cons of each lens and be better able to predict which patient will be best served by a given design. This streamlines the fitting process and increases success rates.
Once you establish an inventory of fitting sets, you will be better able to pre-screen patients. Based on his particular prescription and physical characteristics, you can more easily determine whether a patient is a good candidate for presbyopic contact lens correction and which multifocal design is best. You will be able to better predict the likelihood of needing changes after the initial lenses are dispensed and properly educate patients on the need and rationale for follow-up visits.
Both you and your patient will need patience during the follow-up period as it is not uncommon to require modifications in the distance power, add power or both. Pay careful attention to the patient's complaints and comments which will help you give the patient positive changes to improve visual performance. For best results, use loose lenses during the over-refraction and vary lighting to allow the patient a more natural visual setting.
Professional Fees
Charge appropriately for your services. Consider separating professional fees from material charges and explaining this breakdown so that the patient does not perceive the charge as "just for two contact lenses." Keep the professional fees higher and the material charges lower. This keeps replacement lens costs lower as well as discourages patients from shopping around once the fitting is complete.
Conclusion
Nothing about multifocal or bifocal contact lens fitting is difficult as it is really a progression of standard contact lens practice. As the number of patients needing presbyopic correction increases, provide services that bring them into your office and keep them there.
To receive references via fax, call (800) 239-4684 and request document #76. (Have a fax number ready.)