


prescribing for presbyopia
Motion Is the Potion to Cure Many Gas Perm Bifocal Ills
BY THOMAS QUINN, OD, MS
November 2001
The need for proper multifocal lens movement may seem obvious. We know an alternating bifocal needs to translate properly in order for the patient to see well at distance and near. Appropriate lens dynamics plays a sometimes unrecognized, but undeniably vital, role in many other aspects of oxygen permeable (OP) bifocal lens success. Let's look at the role lens motion plays when fitting alternating and simultaneous vision multifocal lens designs.
Alternating Designs
Proper lens translation occurs when, as the eye moves from a straight ahead to downward gaze, the lens moves up on the cornea to a degree that allows the reading segment of the lens to move into the line of sight and provide clear near vision. Also, in straight ahead gaze the lens must drop quickly following the blink so the add portion of the lens doesn't "hang" in front of the pupil.
Aside from the visual issues affected by alternating design lens movement, physiological response can be impacted as well. The most common adverse response resulting from insufficient lens movement of these prism-ballasted designs is 3 to 9 o'clock staining with associated conjunctival injection. If this problem is observed, consider flattening the lens at least 0.50D. If the problem persists, try decreasing prism, but take precautions to ensure enough prism so the lens continues to drop quickly.
If minimal movement is due to a partial blink, a larger diameter may prove beneficial by increasing lens-to-lid interaction, and subsequent lens movement.
|
|
|
|
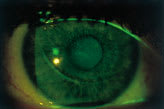
Figure 1. Impression ring and central corneal staining observed following removal of an adherent
lens. |
|
Simultaneous Designs
Minimal movement of simultaneous bifocal designs is desirable for vision stability. Achieve this by biasing the lens-to-cornea fitting relationship a little steep or by utilizing a lid attachment approach. The latter allows the upper lid to serve as a "lens anchor," stabilizing the lens in position along the line of sight.
Though a stable fit is needed to be successful with these designs, some lens movement is necessary to maintain physiological integrity.
Aspheric posterior surface simultaneous vision designs are among my favorite multifocal designs due to their comfort and ability to correct vision for all distances. However, sometimes these lenses develop adherence or non-movement syndrome. This can lead to epithelial compromise (Figure 1), spectacle blur and discomfort, often most pronounced following lens removal.
Some may attribute lens adherence to a lens fit too steeply, creating a suction effect, and attempt to correct this problem by flattening the base curve. However, with these designs in particular, lens adherence can be associated with the aspheric posterior lens surface aligning too closely with the aspheric corneal surface. Such a perfect alignment creates a very thin tear film and subsequent adverse fluid dynamics, which leads to lens adherence. When you see non-movement syndrome, steepen the fit by at least 0.50D to enhance movement.
If you see your multifocal OP patients after only an hour of wear, you may not observe movement maladies. Schedule your patients for follow-up after they have been wearing their lenses for at least four hours.
If the patient is experiencing problems, be it visual or physiological, modifications to optimize movement may be just the right medicine.
Dr. Quinn is in group practice in Athens, Ohio, and has served as a faculty member at The Ohio State University College of Optometry.