


contact lens case reports
The Effect of Corneal Diameter on Soft Lens Fitting, Part
1
BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRE, FAAO
Today many soft contact lenses are available in only one diameter and, at most, two base curves. Manufacturers of mass-produced soft lenses must limit the number of available lens parameters to minimize inventories and so remain competitive in today's frequent replacement market. "Off the rack" soft lenses will fit most prospective contact lens patients, but there are situations that require a lens design outside of the available contact lens parameters.
|
|
|
|
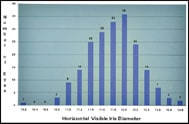
Figure 1. The horizontal visible iris diameters of 200 consecutive right eyes as measured with a precision slit lamp reticule. |
|
All soft lens fitting is based on matching the sagittal height of the lens with that of the anterior eye. The sagittal height of the eye is predicated on five anatomical features: the central corneal radius, overall corneal diameter, corneal asphericity and the radius and asphericity of the para-limbal sclera. All too often, practitioners are instructed to select the appropriate lens radius based solely on central keratometric measurements, yet it is clear that the central radius of curvature plays only a minor role in the overall sagittal height of the eye. For years we have known that corneal diameter dominates as the major contributor to the height of the anterior segment.
In an effort to better understand the diversity of corneal diameter in the population, we measured the horizontal visible iris diameter (HVID) of 200 consecutive right eyes in our contact lens practice. In our study, the average HVID was 11.8mm with a range of 10.2mm to 13.0mm (Figure 1). Figure 2 illustrates the photokeratoscopy and Scheinpflug photography of the two patients on either end of the bell-shaped curve.
|
|
|
|
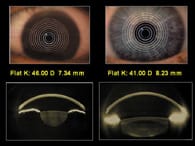
Figure 2 Left, patient MC with a HVID of 10.2mm and right, patient DP with an HVID of 13.0mm. |
The Two Extremes
Patient MC (with the 10.2mm corneas) had Ks of 46.25 @ 180/46.50 @ 90, while patient DP (with the 13.0mm corneas), had Ks of 40.00 @ 180/40.50 @ 90. Based on keratometry, we would expect the steeper corneas of patient MC to require a contact lens with a steeper base curve, but it is clear from the Scheinpflug photographs that the opposite is true.
Ultimately, the patient with the 10.2mm corneas (Ks 46.25 diopters) required a custom soft lens with a relatively flat base curve of 8.8mm and a 13.5mm diameter, while the patient with the 13.0mm corneas (Ks 40.00 diopters) required a custom soft lens with a steep base curve of 8.3mm and a 15.0mm diameter.
In both cases, all of the currently available, mass-produced soft lenses failed to provide the appropriate cornea-to-contact lens fitting relationship.
Patrick Caroline is an associate professor of optometry at Pacific University and an assistant professor of ophthalmology at the Oregon Health Sciences University.
Mark André is director of contact lens services at the Oregon Health Sciences University.