


treatment plan
Corneal Topography
Masquerades Part II
BY TIMOTHY T. MCMAHON, OD, FAAO
This is the second in a two-part column on topographic masquerades. As mentioned last time, one can find plenty of powerful information within a topographic map. However, at times there mixed signals given that can appear as one thing but in reality be something totally different. Adorning this page are two images with similar appearances. They represent two conditions that are reasonably common.
there are mixed signals given that can appear as one thing but in reality be something totally different. Adorning this page are two images with similar appearances. They represent two reasonably common conditions.
|
|
|
|
Figure 1. What is Condition
1? |
|

Condition 1
Figure 1 reveals:
- An axial curvature map with a relative scale using 1.00 diopter intervals
- A notable inferior steepening
- An inferior tear-drop-like pattern
- A maximum curvature of at least 53.50 diopters
- A dioptric contour range across the map of 11 diopters (53.50 to 42.50=11.00 diopters).
Virtually all these features should trigger your warning bells that something is amiss. Inferior steepening and inferior teardrop patterns are rarely found in normal corneas. A maximum curvature of 53.50 diopters has a less than 1 percent chance of occurring in a normal eye, and normal corneas have contour ranges less than 4.50 diopters. As you probably determined on your own, this is a case of an eye with keratoconus.
|
|
|
|
Figure 2. What is Condition
2? |
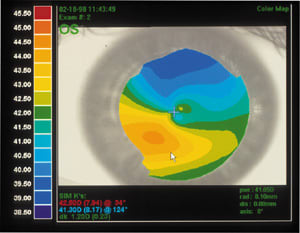
Condition 2
Figure 2 reveals:
- An axial curvature map with relative scale using 0.50 diopter intervals
- Some inferior steepening
- An inferior teardrop pattern similar to that found in Figure 1
- A maximum curvature of 44.50 diopters
- A contour range of 5.50 diopters.
Again you see some alarm triggers in this map, most notably the inferior teardrop pattern and inferior steepening as well as the extended contour range (normal is less than 4.50 diopters).
Is this mild keratoconus? It certainly could be, but as the title suggests, it's not. It's a masquerade. In fact, this is a cornea distorted by a posterior aspheric GP contact lens giving the false appearance of an early case of keratoconus. In this case, the pre lens-wearing topography was normal, and the topography returned to normal after ceasing lens wear.
Farewell
A last comment, this is my swan song for Treatment Plan. It has been a pleasure writing the pieces, and my hope is that you, the reader, have found them valuable. Finally, it has been a pleasure working with the staff of Contact Lens Spectrum and Dr. Barr. Best wishes to you all.
Dr. McMahon is a professor and Director of the Contact Lens Service at the University of Illinois at Chicago Dept. of Ophthalmology & Visual Sciences.