


Extended Wear: Past, Present and Future
By Brien Holden, PhD, DSc,
OAM
January 2002
Extended wear lenses have come a long way over the past 50 years and are now poised to change the contact lens world forever.
Professor Otto Wichterle was a great humanitarian, scholar and scientist. He had many dreams, including peace and freedom for his beloved country, Czechoslovakia. One of his professional dreams was affordable vision excellence for all people. To this end, he was the first to produce an extremely inexpensive molded IOL for cataract patients. Another related ambition was for a contact lens that could be worn by anybody for any length of time. He envisioned a "natural" contact lens that would be extremely low in cost and either disposable or worn all the time. He, and the world at the time, had little understanding of the needs of the anterior eye for relatively high levels of oxygen, but he thought that such a lens must be soft and compatible with the eye.
Thus, 50 years ago, Otto Wichterle formulated the requirements for a material which would have optimum compatibility toward living tissue. To his way of thinking it should:
- Have an elasticity similar to that of the tissue with which it is to come in contact.
- Be permeable for water.
- Be chemically and biochemically stable under physiological conditions.
Wichterle and Drashoslav Lim, working at the Institute of Chemical Technology of the Czechoslovak Academy of Sciences in Prague, proceeded to make and patent such a material. They developed a stable transparent gel, hydroxyethyl methacrylate (HEMA), and filed patents on the material for a wide range of possible applications, including contact lenses. The first HEMA contact lenses were used in their own eyes in 1957, maybe even before. There were legions of skeptics, many scorned his floppy lens, claiming it could not provide optical correction. The new prototype lenses may not have been very comfortable, but according to Wichterle, "I could see my hand clearly, so I knew they would work." He and Lim persisted, and a whole new industry and method of vision correction was spawned from the imaginations of these men.
|
|
|
|
Figure 1. Oxygen needs for
the cornea. |
|

The Holy Grail
Since those first soft lenses, the contact lens industry has seen enormous growth from the research, development and subsequent improvements in soft lens materials and manufacturing technology. In 1970, there were two million contact lens wearers worldwide, mainly PMMA; in 1986, there were 25 million; and today there are nearly 100 million. Despite these improvements, patients are still searching for the ultimate method of vision correction to permanently correct their sight, many now turning to laser surgery or other alternatives.
The keys to patient satisfaction with methods of vision correction have always been convenience, good vision, ocular comfort and safety. Monthly continuous wear has long been the "Holy Grail" of contact lenses. In surveys conducted by the Cornea and Contact Lens Research Unit (CCLRU) and the Cooperative Research Centre for Eye Research and Technology (CRCERT), patients have overwhelmingly indicated their desire for "permanent" vision correction, with 97 percent expressing the desire to be able to wear contact lenses continuously for at least six nights or more. Though patients thought that initial comfort and quality of vision were the most important features in their choice of the contact lens they wore, 85 percent believed that extended wear was an essential feature in choosing contact lenses as a method of vision correction.
The first barrier to a successful extended wear lens was oxygen permeability. Conventional contact lenses invariably reduced the oxygen levels available to the anterior corneal surface, and when worn overnight, closed eyes further reduced the availability of oxygen needed for corneal health.
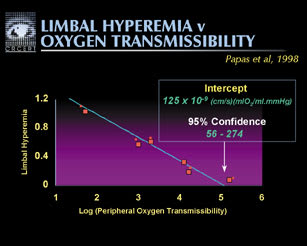
Though a controversial issue for many years, eventually the work of George Mertz, OD, John McNally, OD, and myself defined the levels needed to avoid overnight edema. We established that for contact lenses to achieve an overnight (closed eye) level of edema of 4 percent, the level must have an oxygen permeability (Dk/t) of at least 87 barrers. Interestingly, if we use the average overnight level for no lens edema of 3.2 percent, the average level from all recent studies (La Hood, Fonn), to avoid overnight lens corneal swelling, the Holden-Mertz equation predicts 125 barrers would be needed (Figure 1).
The contact lens industry has tried for the past 30 years to find an effective soft lens material that meets or exceeds this level of permeability. The hypothesis has been that if it were provided, we would see no hypoxic-induced adverse effects on the corneal structure and function that would create a susceptibility to ocular infection.
With silicone hydrogels, we now have such a material, which provides up to eight times the oxygen transmissibility of conventional soft contact lenses while providing similar immediate comfort, fitting performance and surface characteristics to current disposable soft contact lenses.
|
|
|
|
Figure
2. Microcyst levels for low and high Dk lenses. |

Hypoxia and Other Adverse Effects
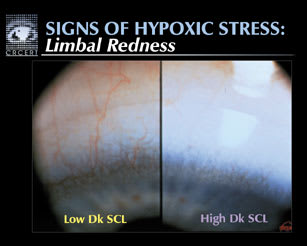
The new highly oxygen-permeable silicone hydrogel materials have eliminated physiological changes due to hypoxia for the majority of patients for higher Dk materials. Overnight edema levels with the new generation materials are similar to the levels seen with no lens wear and are far lower than those with commercially-available disposable soft lenses. Contact lens-induced corneal striae, microcysts (Figure 2) and lens-induced endothelial polymegethism are rarely, if ever, seen with the higher oxygen-transmissible silicone hydrogels. Silicone hydrogel lenses also reduce limbal redness (Figures 3 and 4) and eliminate limbal vascularization experienced by previous wearers of low Dk extended wear lenses, leaving only ghost vessels. The myopic shifts observed with disposable hydrogel extended wear lenses also do not occur with silicone hydrogels.
Studies of adverse responses conducted at CCLRU/CRCERT and the Contact Lens Research Unit (CLRU) of the University of Waterloo with the new lenses compared to low Dk lenses have shown similar rates of inflammatory conditions such as contact lens-induced peripheral ulcers, contact lens-induced acute red eye and infiltrative keratitis.
With other features of the new materials, mainly greater stiffness and less hydrophilic surfaces, some old physical challenges such as superior epithelial arcuate lesions (SEALs) and localized contact lens papillary conjunctivitis have returned and have similar or higher incidence rates to other soft lenses.
|
|
|
|
Figure 3. Limbal hyperemia
vs. oxygen transmissibility. |
|
A Reduced Risk of MK
Of course, the main concern with any extended wear contact lens is the incidence of microbial keratitis (MK). This is the only sight-threatening adverse event associated with lens wear, and it therefore re-quires careful scrutiny.
Conventional contact lenses reduce the amount of oxygen reaching the cornea (Figure 5). With extended wear of low oxygen-permeable lenses, the closedeye environment leads to severe metabolic stress. This stress leads to a thin, attenuated, poorly-metabolizing epithelium. This in turns leads to a high risk of the adherence of pathogenic bacteria to the compromised epithelium, and hence MK.
It is hypothesized that the increased oxygen permeability of the silicone hydrogel lenses creates a healthier epithelium and ensures that the eye's defenses are not compromised, providing better protection against infection.
|
|
|
|
Figure
4. Limbal redness with low and high Dk lenses. |
So far, there have been 13 reported cases of MK occurring with silicone hydrogel lenses in the marketplace out of approximately 350,000 wearers, with about 250,000 wearer-years of experience, one per 22,000 patient years, compared with the currently accepted figure for low Dk soft lens EW of one per 500 patient years.
We always knew that MK would occur with high Dk soft lenses. While products are designed to be safe, we know that not all our patients will be compliant all the time. We also do not know just how much additional protection eliminating hypoxia provides. Some patients will be at risk of infection, despite high Dk.
EW Vs. LASIK
None of the high Dk MK cases have lost two or more lines of best corrected visual acuity (BCVA). Compared to refractive surgery, this is an excellent result. Currently, the rate of loss of two lines BCVA for LASIK is one in 32, compared to one in 12,024 for low Dk extended wear contact lenses, and one in 37,991 for all contact lenses, according to the studies of Cheng and colleagues.
The only possible serious adverse event with contact lenses is MK. Serious adverse events associated with LASIK include:
- MK
- Loss of vision due to severe aberrations
- Loss of vision due to surgical complications
- Corneal ectasia
- Lamellar keratitis
- Severe, debilitating dry eye
- Retinal detachment
- Bilateral keratitis
- Bilateral optic neuropathy
- Bilateral macular hemorrhage
Up to five percent of patients may have a range of less serious, but still concerning, problems following laser surgery. Unhappy patients of laser procedures report:
- Residual hypermetropia or myopia, meaning that vision may still need to be corrected
- Haloes at night (blurriness around lights)
- Myopic regression, where eyesight changes back to the original refraction
- Monocular diplopia, or double vision
- Decreased contrast sensitivity
- Dry eyes
- Nighttime driving difficulties.
It seems clear that high Dk extended wear lenses have much lower risks than surgery while still meeting patients' desire for the convenience of constant vision without ocular discomfort.
|
|
|
|
Figure
5. Corneal swelling with
hydrogel and silicone hydrogel lenses. |

Practitioner Fear
Despite the positive physiology, the interest of the public in such lenses, the publicity surrounding their launch and wearer enthusiasm, practitioners' fear of complications is still having a marked influence on the market.
Recent practitioner surveys at conferences in Britain, Australia and Sweden show that fear of infection and adverse responses are significant inhibitory factors with regard to extended wear, because of the previous poor history of this modality. Practitioners' lens of first choice for uncomplicated myopes is still overwhelmingly daily wear, especially daily disposable lenses.
Patient Enthusiasm
CCLRU/CRCERT patients who have worn silicone hydrogel lenses successfully for 12 months or longer report overwhelming satisfaction, with 93 percent rating the lenses as excellent. The main reasons for their satisfaction with the continuous wear system were the elimination of the need for care and maintenance and lens handling (88 percent), being able to see in the morning (7 percent) and excellent comfort (5 percent). Ten percent of patients reported that they forgot that they were wearing lenses at all.
Prior to trying continuous wear, two-thirds of these patients had considered refractive surgery to permanently correct their vision. Following their continuous wear experiences, only 32 percent of these patients would still consider refractive surgery "even if it were perfect." Once continuous wear has been successfully experienced, patients strongly prefer it as a form of "permanent" vision correction. Similar results were found in surveys at the CCLR in Canada.
In Australia, there has been a strong market response to the launch of high Dk lenses. They captured five percent of the contact lens market in their first year, and we have since seen a doubling in the silicone hydrogel market every 12 months. Currently over 30 percent of patients returning for contact lenses are shifted to silicone hydrogel lenses.
How To Make EW a Reality
First, in order to assess in the real world how well this new generation of contact lenses is performing, we need to accurately define the MK rate. We are attempting to mount a benchmark study with our national and international colleagues as a matter of some urgency. Practitioners will then be able to review the results, listen to the experience of their colleagues and, if satisfied, try it for themselves and their patients. The most important thing is for practitioners to be well informed and to develop the attitude that silicone hydrogels should be tested as a way of fulfilling the needs and desires of their patients for convenient, effective continuous vision. Practitioners need to be willing to gain firsthand experience before making a decision about this new modality, as it will be proven only in the public arena. Finally, both the practitioner and the patient need to be aware of the signs and symptoms of adverse responses, to recognize that they are treatable or manageable, and that patients must check their eyes every day in order to minimize risk. Patients should ask themselves, as Stan Yamane, OD, once said, "Do my eyes look good? Do my eyes feel good? Do my eyes see well?" If the answer is "no" to any of these questions, they should contact their eyecare practitioner.
Looking Ahead
FDA approval of silicone hydrogel extended wear lenses will have a significant effect on the marketplace, not only in the United States but all over the world. With maybe 500,000 wearers by year end 2002, and doubling each subsequent year, extended wear will continue to make an impact in the contact lens market as patients search for more convenient and safer forms of "permanent" vision correction.
We will monitor the results of extended wear in terms of patient safety. Accurate measures of adverse response rates will be important in addressing practitioner fears and in ensuring the safety and efficacy of this new form of vision correction.
While practitioners are still coming to grips with new high Dk extended wear, researchers are already working on the next generation of products. New designs and surfaces are undoubtedly on the drawing boards to address the current issues with silicone hydrogel lenses.
In the survey of patient satisfaction at CCLRU, the most frequent disadvantages of extended wear lenses were discomfort, dryness and that many patients wanted to be able to wear their lenses for even longer than one month. Approximately 10 percent of the group surveyed listed deposits as a disadvantage of their current lenses. Problems with deposits, which can interfere with the quality of vision and require the lenses to be removed and cleaned, need to be overcome or reduced. These results indicate the need for further development in the area of true compatibility with the eye.
Conclusion
Contact lenses are going through an extremely interesting stage. Over the last 10 years, hundreds of millions of dollars have been invested to try to perfect them. Extended wear contact lenses have the potential to change the lives of many people around the world who need vision correction, offering continuous vision with comfort and convenience. Clinical studies have shown both excellent objective physiological results and patient enthusiasm for the lenses. However, practitioners still need to educate patients about appropriate eye care and to ensure that patients remain vigilant about their ocular health. At the same time, researchers and industry are seeking new levels of biocompatibility and comfort in an attempt to make contact lenses that are superior to and more convenient than spectacles. Time will tell whether contact lenses can achieve the compatibility needed to realize their full potential.
The author would like to acknowledge the help of Kylie Evans in writing this update and a host of colleagues at the CCLRU and CCLR for their input.
To receive references via fax, call (800) 239-4684 and request document #78. (Have a fax number ready.)
