


orthokeratology today
Parameters of Reverse
Geometry Lens Designs
BY CRAIG W. NORMAN, FCLSA
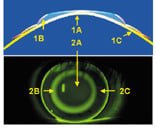
Unlike typical multicurve rigid gas permeable (RGP) lenses, which are steep in the center and flatten progressively towards the periphery, reverse geometry lens designs have a flat central base curve (1a, 2a), then a significantly
curve (Figures 1a, 2a), then a significantly steeper reverse curve zone (Figures 1b, 2b), an alignment area that is steeper than the base curve (Figures 1c, 2c), then a flat posterior peripheral curve zone. Each part of the lens plays a role in the corneal reshaping process of orthokeratology.
While each of the reverse geometry lens designs available today have proprietary components to them, there are more similarities than differences among them.
|
|
|
|
Figures 1 and 2 show the different zones of a reverse geometry
lens. |
|
Base Curve
The base curve area induces desired myopic reduction changes. Generally, the radius of curvature should be flatter than flat K by an amount 0.50D to 0.75D greater than the refractive change desired. For instance, if the amount of myopia is 3.00D, select a base curve radius 3.50D to 3.75D flatter than K; the resultant lens power will be +0.50D or +0.75D. This power, termed the Jessen Factor, allows for any potential regression of myopic refractive error during the day.
While the diameter of this zone can vary, it is small in comparison to traditional RGP designs, usually 6.0mm in size. A smaller diameter might increase the ortho-k effect, but it also increases the chance of such optical disturbance as haloes and glare during waking (non-wearing) hours. Larger OZ diameters reduce the corneal change effect.
Alignment Curve
One orthokeratology fitting goal is to design a lens that remains centered and provides a treatment zone directly over the pupil. The alignment/fitting curve (landing zone) is key to achieving this goal because it controls lens movement and lens positioning. This zone may be spheric, aspheric or, in some designs, have a cone angle, which is a straight line set at an angle tangent to the portion of the cornea it touches. Subtle changes in this zone can significantly impact contact lens centration and improve treatment results.
Reverse Curve
The reverse/relief curve serves two important functions. First, it is designed to connect the base curve and alignment curve without altering their relationship to the cornea. Secondly, the central corneal epithelium is redistributed to this area during treatment. This area can vary in size and depth from one design to another, ranging from significantly steeper than the base curve or, in one proprietary design, a sigmoidal curve to connect the base curve and alignment areas.
Peripheral Curve
The peripheral curve serves the same purpose in reverse geometry lenses as in standard RGP lens designs in that it provides a tear reservoir while aiding tear circulation. This zone is usually 0.4mm in width, with a radius of 10.0mm to 12.25mm. In designs that employ cone angles, a peripheral curve may not be necessary.
Visit www.clspectrum.com for information on the Global Orthokeratology Symposium in Toronto.
Craig W. Norman is Director of the Contact Lens Section at the South Bend Clinic in South Bend, Indiana. He is a fellow of the Contact Lens Society of America and an advisor to the RGP Lens Institute.