


orthokeratology today
Can Orthokeratology Correct
Astigmatism?
BY JOHN MARK JACKSON, OD, MS, FAAO
Orthokeratology may affect astigmatism. Prior to reverse geometry (RG) lens fitting, lenses would often decenter superiorly and distort the cornea, resulting in increased with-the-rule astigmatism. Modern RG designs reportedly do not cause this effect, and may reduce astigmatism as well.
|
|
|
|
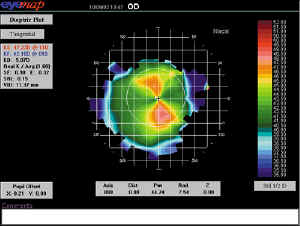
Figure 1. Centrally located astigmatism
"bowtie." |
|
Modern RG designs reportedly do not cause this effect, and may reduce astigmatism.
Little research supports this claim. Most studies report changes in the spherical equivalent without reporting cylinder changes. The studies that discuss astigmatism have often reported only an average change in cylinder power without taking axis direction into account, leading to inaccurate conclusions.
At the Global Orthokeratology Symposium in Toronto in August 2002, several papers were presented regarding astigmatism changes using these methods.
Power Vector Analysis
The LOOK (Lenses and Overnight Orthokeratology) Study group at The Ohio State University presented data from their pilot study using Power Vector analysis to examine astigmatism changes. Power Vector analysis is a new way to examine both the amount of astigmatism change and the direction. They found no significant change in mean cylinder and axis from baseline, meaning that the procedure (using RG lenses) neither increased nor decreased astigmatism on average. However, the average astigmatism at baseline was only about 0.50DC, which may have affected the analysis.
|
|
|
|
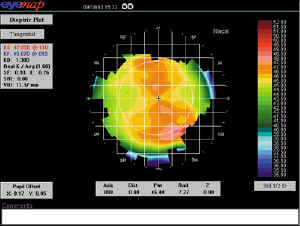
Figure 2. Limbus to limbus astigmatism. |
|
Bowtie Topography
Dr. John Mountford from Australia presented a study that used a similar method of vector analysis, but with different results. This study identified a difference in astigmatic changes based upon the extent of astigmatism across the cornea visible on topography. When the "bowtie" was confined to the central pupillary zone (Figure 1), the astigmatism decreased on average by about 50 percent. When the "bowtie" extended beyond the pupillary zone toward the limbus (Figure 2), astigmatism increased on average; a spherical RG lens design was unable to correct this type. He concluded that the location and amount of the astigmatism is an important baseline predictor of success; clinicians should look for centralized astigmatism of less than 1.50DC for greatest chance of success.
For the more difficult cases, a more radical lens design will be needed. Dr. Michael Baertschi from Switzerland presented initial work in designing toric RG lenses. The goal for this design is to improve centration and stability on toric corneas and to improve the corneal correction. His early work has shown improvement in lens stability but not in optical correction.
Dr. Jackson is an assistant professor at Southern College of Optometry where he works in the Advanced Contact Lens Service, teaches courses in contact lenses and performs clinical research.