


treatment plan
Acanthamoeba Keratitis
BY WILLIAM MILLER, OD, PHD, FAAO
Acanthamoeba is a rare but potentially devastating ocular infection. Although first reported nearly 30 years ago, its numbers have increased, perhaps due to better detection methods or the influence from environmental factors (contact lenses, hot tubs, etc.) The incidence of Acanthamoebic keratitis has been reported as 33 per million contact lens wearers and about 20 per million in Hong Kong and England, respectively. This number is typically significantly (20-fold) higher than in the non-contact lens wearing population. In the United States, the incidence is much lower (1.36 per million) than reported in Hong Kong and England; however, even in England, incidence rates vary widely geographically.
Acanthamoeba is a water-borne protozoa existing in two forms; trophozoite and cyst. Its trophozoite form is active, exhibiting curled spider-like pseudopodia. In the presence of an adverse environment, the protozoan can protect itself by turning into the cyst form, which is smaller than the active trophozoite and sports a double-walled envelope. A small compromise in the corneal epithelium revealing mannose-containing glycoproteins represent points of adhesion with an eventual open invitation for Acanthamoeba invasion.
|
|
|
|
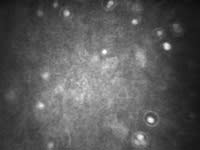
Figure 1. Corneal Acanthamoebic cysts as viewed through in-vivo confocal
microscopy. |
|
Signs and Symptoms
Symptoms of Acanthamoeba keratitis include a unilateral red eye combined with pain, photophobia, foreign body sensation and epiphora. A key component, although not pathognomonic, is the relative disparity between severe symptoms and mild signs.
Signs may include dendritiform epithelial lesions which may progress to ulceration with eventual opacification. Less diagnostic signs such as conjunctival hyperemia and blepharospasm are also present. Stromal ulceration may show a ring or partial ring of infiltrates, raising the suspicion of Acanthamoeba. The infiltrative process can also run linearly along corneal nerves, displaying the characteristic radial keratoneuritis, truly pathognomonic for this keratitis. Iritis may also be present. Left to its own devices, these virulent protozoa can cause corneal perforation.
Most of the devastating effects of Acanthamoeba result from a delay in diagnosis. This delay is often due to its similarities with other forms of ulcerative keratitis, including herpes simplex and herpes zoster. Other methods to isolate the diagnosis include the use of light microscopy via corneal culturing or biopsy. Corneal tissue acquisition with subsequent staining with calcofluor white is necessary for diagnosis. Recent developments in clinical in-vivo confocal microscopy to image and distinguish between Acanthamoebic cysts and trophozoites have provided the clinician with a useful tool in arriving at a definitive diagnosis.
Treatment
Current treatments for Acanthamoeba consist of antifungals (fluconazole or clotrimazole), cationic antiseptics (polyhexamtheylene biguanide [PHMB] or chlorhexidine), diamides (propamidine) or aminoglycosides (neomycin). A recent strategy is to combine medications for an Acanthamoeba cocktail, which may consist of chlorhexidine or PHMB and propanidime given every hour for the first few days, followed by the same combination given every two hours for the next three days. A maintenance dosing of PHMB or chlorhexidine then continues over the next three to four months
Dr. Miller is on faculty at the University of Houston College of Optometry. He is a member of the American Optometric Association and serves on its Journal Review Board. He can be reached at wmiller@uh.edu.