


therapeutic topics
Going Off Label
BY WILLIAM TOWNSEND, OD
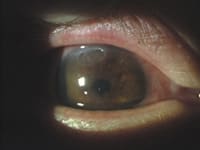
Traci, a 33-year-old female, presented with discomfort and a gradually worsening, slight decrease in vision in her right eye. Her left eye had poor vision from a previous "abrasion" that another eyecare provider had managed. Her general history was significant for allergy, asthma and recurrent dermatitis. Presenting acuities were OD 20/50, OS 20/400. Gross external evaluation revealed dry, scaly patches of skin on the eyelids, cheeks and popliteal flexures. Biomicroscopy OD showed punctuate keratitis and a horizontal ulcer in the superior right cornea (Figure 1). The left eye had stromal neovascularization involving the superior cornea and visual axis. Eversion of the eyelids revealed multiple giant papillae OU.
We diagnosed atopic keratoconjunctivitis (AKC) with a shield ulcer OD and prescribed Lotemax (Bausch & Lomb) q2h and a combination mast cell stabilizer/antihistamine q6h.
|
|
|
|
Figure 1. AKC caused punctuate
keratitis and a shield ulcer OD. |
|
Trying Something New
We continued this protocol for several days without appreciable improvement. We then opted to add cyclosporine 0.05% emulsion (Restasis, Allergan) q12h. Within 24 hours, we noted improved vision (20/30) and overall eye appearance. Over the next weeks, we tapered the steroid, maintained the cyclosporine and encouraged Traci to use non-preserved artificial tears on a regular basis. At her last visit, the shield ulcer had healed with minimal scarring and best corrected vision OD was 20/20.
Understanding Treatment
Effective disease treatment involves understanding the disease and the mechanism of drugs we prescribe. Atopic dermatitis occurs in three percent of the population, and 15 percent to 40 percent of those affected will develop AKC. It involves Type I and Type IV hypersensitivity and is associated with IgE-mediated eczema. T-helper cells also contribute to AKC. Allergens such as house dust mites, mold spores and animal danders may exacerbate the condition.
In Traci's case, we added cyclosporine because of its immunomodulatory effect on T-cells. It enters the cell passively and inactivates lymphocytes that produce interleukins and interferon gamma. Corticosteroids and mast cell stabilizers theoretically block the immunologic effects of the cells that contribute to AKC, but steroid-resistant AKC does exist (Akpek et al, 2004).
Off-Label Guidelines
When you use a drug for off-label application, be certain that you have justification for doing so. Follow these simple guidelines in case you must later defend your decision to go off label:
- Find adequate scientific evidence to support your decision. (I've already discussed why cyclosporine was appropriate in Traci's case)
- Try approved treatment regimens before going off label. We had to acknowledge failure of Traci's initial treatment plan and pursue other alternatives
- Consider the severity of the situation. We became convinced that the pannus in the left eye resulted from a previous episode of AKC rather than an abrasion. Traci had already lost vision in one eye and was certainly at risk for that happening in the remaining eye if our treatment failed
Scientific data, failure of conventional therapy and the underlying circumstances surrounding the case must ultimately support your off-label decision.
To obtain references for this article, visit www.clspectrum.com/references.asp and click on document #110.
Dr. Townsend is in private practice in Canyon, Texas, and is an adjunct professor at UHCO. E-mail him at drbill1@cox.net.