


orthokeratology today
Using Orthokeratology
To Correct Presbyopia
BY JOHN MARK JACKSON, OD, MS, FAAO
Orthokeratology may be an appropriate corrective option for both young and old myopic patients. But for presbyopic patients, you need to add an extra step in the fitting process because you also need to correct their near vision.
Currently, no "multifocal" lens designs exist for ortho-k, so your options are limited to reading glasses or monovision. Either can work well for your patients, but only monovision can provide them with device-free correction during the day, which is the obvious goal of ortho-k.
|
|
|
|
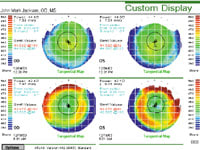
Figure 1. Pre- and post-monovision
ortho-k topography maps. |
|
Getting Started
Begin monovision ortho-k treatment by selecting the near eye as you would for a standard monovision contact lens fitting (determine eye dominance, etc.). Design your lenses as you normally would for full distance correction, then modify the lens for the near eye by altering the base curve (BC). Steepen the BC by the amount of add power required.
For example, if the distance calculation results in a 43.00 diopter (7.85mm) BC, and you need a +1.00D add, then steepen the BC to 44.00 diopters (7.67mm). This should undercorrect the near eye by the desired amount. You may need to alter the reverse curve and/or alignment curve to maintain the appropriate lens sagittal depth.
After the patient has worn the lenses and you achieve the full ortho-k effect (Figure 1), modify the lens design to "tweak" the treatment if you didn't achieve the desired outcome.
A Wait-and-See Approach
Steven Shum, OD, of Germantown, TN recommends a slightly different approach. He initially targets full distance correction in both eyes and asks the patient to wear those lenses for two weeks. After treatment has reached its maximum, if one eye remains slightly undercorrected, then he selects that eye for near and makes the appropriate adjustment to reach the desired near correction in that eye. This provides the added benefit of letting the patient compare both full distance and monovision correction.
Balancing the Near Correction
The patient's baseline refractive error may help you determine which eye to use for near. If the patient already has close to the desired add in one eye (for example, a 2.00D myope who needs a +2.00D add), then consider treating only the other eye for distance.
If the patient has one eye that is significantly more myopic than the other (for example, 1.50D OD and 3.00D OS), then you'll increase your chance for success if you choose the more myopic eye as the near eye. Using this eye will also allow for better near correction over time, because you can more easily change the amount of treatment with new lenses as the patient's add power increases.
Not for Everyone
Some patients feel that their acuity isn't as crisp with ortho-k monovision as it is with standard lens wear. This may result from mild optical aberrations that the procedure induces.
When both eyes are corrected for distance, binocular summation enhances the visual acuity. This summation doesn't occur with monovision and therefore can cause a decrease in visual quality.
Dr. Jackson is an assistant professor at Southern College of Optometry where he works in the Advanced Contact Lens Service, teaches courses in contact lenses and performs clinical research.