


orthokeratology today
Ortho-k for a Decentered
Corneal Apex
BY JOHN MARK JACKSON, OD, MS, FAAO
Predicting individual success when fitting orthokeratology has always been an issue. Identifying good candidates at the outset will help you maximize your success with this modality. While it's important to know the baseline refractive error, a patient's pre-lens wear corneal topography also has an impact on the treatment effect.
|
|
|
|
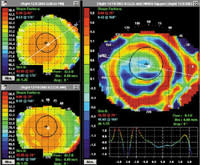
Figure 1. Corneal topography reveals that the lens settled over the decentered corneal apex. |
|
A Pre-Lens Wear Red Flag
One potential troublemaker is a corneal apex that's decentered before treatment. For ortho-k to work, the lens must center over the pupil during wear. Lenses tend to drift to the location of the corneal apex; if the apex is not centered, then the lens will not center either, and an inadequate treatment will likely result.
An Illustrating Case
Patient AH is a 24-year-old female who sought ortho-k treatment because she was tired of wearing soft lenses during the day. Her initial refractive error was 2.50 0.25 x180 OD and 2.50 sphere OS, both to 20/15. The upper left map in Figure 1 shows her baseline corneal topography.
While she was a good candidate based on her refractive error, her corneal apex was shifted inferior-temporally in each eye (her corneas were otherwise normal). Not knowing any better at the time, I fit her with a pair of ortho-k lenses.
The bottom left map shows the one-day result from the right lens, and the far right map shows the difference or change from baseline. You can see that the treatment area decentered inferior-temporally, indicating that the lens centered over the corneal apex. The left eye treatment resulted in a similar effect.
Sometimes an inferiorly decentered treatment area results when the lens sag depth is too deep, so I next tried a shallower sag depth. The result was the same. I discontinued treatment at that point in time, and AH returned to soft lens wear.
Don't Give Up
The GP lab I used for this lens fit was helpful in identifying the cause of AH's problem. The lab representative also suggested that I try a larger diameter lens in cases in which the patient has a decentered corneal apex. I've since fit two other patients with similar cases in which a larger diameter lens resulted in good centration.
Screening for Success
Ortho-k can be a beneficial modality for the right patients. Be sure to carefully screen each candidate before fitting to look for potential fitting pitfalls. Doing so will help you maximize your success.
Dr. Jackson is an assistant professor at Southern College of Optometry where he works in the Advanced Contact Lens Service, teaches courses in contact lenses and performs clinical research.