


LENS DESIGN
Dual Geometric Lenses for Hyperopia Ortho-K
A new type of ortho-k lens promises to be less complicated and more successful.
By Hsiao-Ching Tung, MD, FIOS
Modern ortho-k for myopia reduction is effective and well-known to eyecare practitioners. However, many doubters believe that orthokeratology is a vague and difficult approach to managing hyperopia.
A traditional method of managing hyperopia is to apply a series of progressively steeper GPs, trying to push the cornea tissue inward for piling up at the central portion of the cornea. For this purpose, you should choose a GP that's small in diameter and fit it steeper in stepwise to prevent it from causing adverse effects.
With such a complicated procedure, the result for treating hyperopia is still unremarkable and unpredictable. Often the tissue piles up at the midperipheral portion instead of at the central portion of the cornea, which in turn flattens the central cornea curvature and increases the hyperopia.
|
|
|
|
Figure 1. Dual geometric lens. |
|

Going Against Tradition
The concept of the dual geometric lens is a reverse thinking of the traditional ortho-k for hyperopia.
Here's the hypothesis:
1. We have to prevent tissue from piling up at the midperipheral area when trying to push the tissue all the way into the central portion of the cornea.
2. It might be much easier to flatten the midperipheral portion of the cornea to enhance the steepening of central cornea than merely trying to steepen the central cornea directly.
Reverse-Thinking Concept
The above thinking processes point to a lens design that should inhibit the piling up of the cornea tissue on the midperipheral cornea and would be even better to help remove the tissue from this portion of the cornea.
This new ortho-k lens (US patent #6,652,095) is called a dual geometric lens. (It's named after the interweaving shape of the curvatures.)
The new dual geometric lens has a central optical zone that's steeper than the central cornea, followed by a narrow band of flatter curvature called the plateau zone, coupled with a series of consecutive curvatures for tear circulation and lens centering (Figure 1).
The dual geometric lens is then matched to the individual cornea by the same principle of sagittal depth calculation in myopia ortho-k.
|
|
|
|
Figure 2 The difference map of a 6-year-old girl with accommodative ET. The eyes were straightened after molding for one week. |
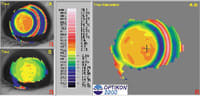
Significant Hyperopia Reduction
When a practitioner fits the lens on the cornea, he should see a typical bulls-eye fluorescein pattern similar to the modern myopia ortho-k, except with central pooling. The effect of the dual geometric lens is far more effective, predictable and maintains its effect longer than the traditional method of ortho-k.
The topography map in Figure 2, which shows a +3.87D reduction in hyperopia, is from a 6-year-old girl with accommodative esotropia.
She was intentionally over-treated with the dual geometric lens to achieve slight myopia to straighten her eyes for reading. Her eyes appeared quite straight after being molded for one week.
Working with the Lens
Practitioners working with hyperopia ortho-k will find that it's quite different from working with ortho-k for myopia. The flatter second zone may cause a ghost image smaller in size accompanying the larger central clear image. For the dual geometric lens for hyperopia, we enlarged the optical zone and smoothed out the shape of the plateau zone to minimize this adverse effect. It is critical to design each peripheral curvature to prevent adverse effects.
For all our ortho-k lenses, including those for myopia, we use a standardized fitting system. The system utilizes a simple reference chart for lens selection. Practitioners can use subjective spherical equivalents and mean corneal curvature measurements to choose the proper lenses.
The system follows the Reverse Z rule: downward and leftward will tighten up the lens while maintaining the same base curve for targeted power. Upward and rightward will loosen the lens while maintaining the same base curve for targeted power.
The system allows practitioners, even those who have limited experience, to fit the lenses easily. The fitting set allows practitioners to make lens adjustments and dispense new lenses on the same day if they choose.
Night wear is recommended, but day wear is also permitted. For night-wear patients, practitioners should follow-up on the first day after night wear, and then again at one week and two weeks. For patients wearing the lenses during the day, practitioners should follow-up on the lens movement six to eight hours after day wear to make sure there is no seal-off.
For both day and night wear, it usually takes one to two weeks for the shape to stabilize.
A central lake may appear, but if it persists longer than three weeks, practitioners need to relieve the central pressure.
For other problems that may occur, such as loose fit and decentration, practitioners may consult the troubleshooting guide for myopia ortho-k.
New Ortho-K Advancements
The dual geometric lens might also be effective for reversing the iatrogenic hyperopia (over treatment) post refractive surgery. We have a patent pending for ortho-k to mold the altered cornea for medical purposes. We are also developing the ortho-k system to manage presbyopia, and also a lens for keratoconus.
A More Effective Lens
When working with the new dual geometric lens, practitioners should observe the patient for long-term effect. However, this new lens has proven to be far more effective than the traditional method of reducing hyperopia.
Editor's Note: Overnight lens wear is not FDA approved for all lens types and may be considered off-label use.
