


MANAGING KERATOCONUS WITH GPS
Using GPs to Manage Keratoconus
Find out why these lenses are an excellent option for satisfying this challenging patient category.
By Joseph Barr, OD, MS, FAAO, Editor and Edward S. Bennett, OD, MSEd
Keratoconus remains one of the most interesting, yet challenging, conditions to manage. The results of the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study have greatly aided our knowledge of this condition. However, much variability exists in the location, progression and corneal changes both between patients and within the same individual. Although keratoconus can begin at almost any age, it progresses faster in a young person (a teenager) than in someone older.
Keratoconic individuals most likely have a genetic predisposition for the condition. In addition, approximately one-half of them have an allergy history, which is at least twice as common as with non-keratoconic individuals, and they typically experience more ocular pain, even without contact lens wear. Certainly practitioners should discourage any trauma to the eye via eye rubbing. The literature suggests that any contact with the apical epithelium causes damage to the underlying stroma when the epithelium is compromised. It's best to advise keratoconic individuals who experience allergies and who tend to rub their eyes to restrict their rubbing to the nasal canthus and not their cornea and, if symptomatic, to use non-steroidal anti-inflammatory drugs (NSAIDs) or mast cell stabilizer/antihistamine combination drugs.
|
|
|
|
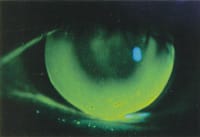
Figure 1. GP contact lens fit on moderate keratoconus eye with definite apical touch, moderate corneal staining and high edge lift. (bubbles are unacceptable) |
|
Whereas a corneal topographer is beneficial when managing keratoconus, it's not required. The benefits are numerous, however, including in the diagnosis, fitting and follow-up care of patients exhibiting this condition. The simulated fluorescein patterns that the software generated with many of these instruments are beneficial, although with the high amount of irregular astigmatism often present, these patterns can vary in their accurate representation of the fitting relationship. The ability to evaluate the actual fluorescein pattern of a lens on the eye is most important to patient success with contact lenses.
Choosing a Material
GP lenses are typically the modality of choice and approximately 90 percent of keratoconic patients who wear contact lenses wear GPs. It's usually advisable to begin with GP lenses and to use other options (piggyback, hybrid, penetrating keratoplasty) when these prove unsuccessful.
The best materials are typically the mid-Dk fluoro-silicone/acrylates (F-S/A) lenses. In addition, high minus refractive error patient could benefit from a high-Dk F-S/A material. Certainly the new mid-to-high Dk GP materials appear similar in their stability and wettability as the old, low-Dk materials.
What About a Trial Fitting Set?
It's imperative to fit keratoconic diagnostic lenses. In fact, the successful fitting of contact lenses for keratoconus often comes as a result of trial-and-error in which the fluorescein pattern dictates what change is necessary. The individual trial sets don't vary all that much (overall/optical zone diameters decrease as the base curve radii steepen). The primary author recommends the CLEK trial set, particularly in early cases of keratoconus. It's available in an 8.6mm/6.5mm overall diameter/optical zone, an 8.5mm secondary curve radius and an 11.5mm peripheral curve radius. However, more similarities exist than differences with the keratoconic lens designs available today and it's important to simply find a design you're comfortable with and stay with it.
The Contact Lens Manufacturers Association lists its keratoconic lens designs in the product guide available at www.rgpli.org.
Approaching the Fit
It's important to strive for either slight apical clearance or mild apical touch. A good initial step is to start at the steeper keratometry reading or, if you're using a topographer, the curvature of the apex on a sagittal map. Evaluating the fluorescein pattern will dictate whether a change is indicated. Good --bordering on slightly excessive -- edge clearance is desired to minimize the likelihood of peripheral sealoff and adherence.
There appears to be no evidence that an excessively flat lens-to-cornea fitting relationship will slow the progression of this condition and, in fact, the resulting trauma may encourage epithelial erosion. It's important to remember that patience is a virtue and it may take several lenses to achieve the best fitting relationship.
|
|
|
|
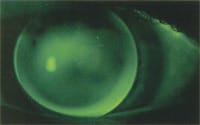
Figure 2. Minimal apical touch to alignment GP lens on
early keratoconus eye, mild debris behind optic zone and moderate edge lift. |
What About Lens Design?
As mentioned previously, the primary author (JB) often begins with an 8.6mm overall diameter with a steep base curve radius; if this isn't successful, he uses a larger diameter with a flatter base curve radius.
The co-author (EB) will often use an 8.8mm to 9.0mm diameter in early to moderate keratoconus (mean keratometry values between 45D and 55D) and 8.0mm to 8.2mm in advanced keratoconus. The optical zone in this philosophy would often be equal to the base curve radius in millimeters (if the base curve radius is 7.0mm, the optical zone would be similar to this value). Regardless of the philosophy, an ultrathin design is recommended to optimize centration. In addition, the use of a plus lenticular or similar peripheral design to optimize edge thickness is recommended in most cases because of the otherwise thick edge inherent with high minus lenses. A peripheral curve radius of, at minimum, 11mm (often 11.5mm to 12.0mm) at a width of at least .3mm will help ensure sufficient edge clearance.
Patient Reactions to GP Lenses
Adaptation may be more challenging to the keratoconic than the non-keratoconic patient for many reasons. Certainly, with the exception of the early keratoconic, an alignment fitting relationship will be absent, making it likely that more edge contact with the lid is present, increasing initial awareness. Likewise, if the lens is decentering, greater awareness is possible.
Finally, it's likely that contact lenses (specifically GPs) weren't a modality that the patient requested, but were recommended for therapeutic purposes by his prescribing practitioner. Therefore, patient motivation may not be optimum in many cases and is exacerbated by the fact that the patient's initial experience with GP lenses is often with a diagnostic lens that doesn't approximate his indicated correction and, therefore, the most important benefit of GP lenses -- good quality of vision -- isn't present. Using a topical anesthetic before the initial application in combination with prescribing a longer-than-average adaptation period will assist in achieving successful adaptation.
Follow-Up Pearls
You should evaluate keratoconic patients weekly until you achieve and sustain an acceptable lens-to-cornea fitting relationship. Ultimately, you should evaluate patients every six to 12 months.
The ability to clean and polish these lenses is important. Specifically, the back surface can easily become deposited, necessitating laboratory cleaning and occasional polishing of this surface. In-office modification of GP lenses is important in keratoconus, not only for polishing but also for flattening and/or blending the peripheral curve radii to allow for adequate tear flow and minimize the risk of peripheral sealoff and adherence.
Piggyback and Hybrid Lens Designs
Whereas spherical GP lenses are almost always the preferred initial option, in cases in which the patient is unable to successfully adapt and also when optimum centration isn't possible, a piggyback modality (a hyper-Dk GP lens material fit over a silicone hydrogel lens) is recommended. With this, as compared to previous generation materials, we've experienced hypoxia-related complications. If this isn't successful, then the Flexlens (Salvatori), which consists of a soft lens with a thinner central depressed area for a GP lens to fit into, is a viable option. The current generation of hybrid materials (Softperm, CIBA Vision) tends to fit tight and may result in a moderate hypoxic corneal response.
What About Lens-Induced Complications?
A whirl or swirl-type of corneal staining isn't uncommon in keratoconus. This is associated with chronic central corneal damage, which can often be associated with the fitting relationship. Practitioners can minimize this through regular follow-up care and possible refitting, if indicated. Most keratoconic patients have staining which, in part, can be associated with a fragile apical region in combination with the presence of a foreign body (a GP lens) in contact with the area. Additionally, they're prone to overwearing the lenses because of the greatly reduced vision they can obtain with their spectacles. It's important to clear up the staining but only refit the patient if a poor lens-to-cornea fitting relationship exists.
A related complication is the presence of a recurrent corneal erosion or a central raised lesion or hypertrophy-proud nebula. This is often the result of either a deposited back surface, an apical bearing fitting relationship or simply the fact that some corneas are more prone to staining.
Summary
GP lenses are an excellent option for managing keratoconus and practitioners can use this option as well as piggyback and scleral lenses surgery in the form of penetrating keratoplasty is a last option. The GP Lens Institute has several educational resources available (videotapes, management guides) to assist in the management of these challenging patients. It's important to note that you're often not going to achieve a "perfect." The key to a successful GP lens fit in keratoconus is to provide good vision, acceptable comfort and good tissue tolerance. In a survey to experienced irregular cornea fitters about fitting such challenging cases, their most common answer was, "Whatever works." In other words, you need to know all of the options and be willing to try them in the patient's best interest.

|
Dr. Bennett is an associate professor of optometry at the University of Missouri-St. Louis and is executive director of the GP Lens Institute. |

|
Dr. Barr is editor of Contact Lens Spectrum. He's a professor and associate at The Ohio State College of Optometry. |