


ASPHERIC LENSES
Aspheric Contact Lenses: Fact and Fiction
An examination of whether soft aspheric contact lenses can correct astigmatism and spherical aberration.
By Pete Kollbaum, OD, FAAO and Arthur Bradley, PhD
Practitioners have used aspheric lenses for a long time to increase the depth of focus of the eye (multifocals). More recently, manufacturers have designed "aspherics" to correct for spherical aberration (SA) of the lens and/or the eye.
In addition to their sphere refractive power, all spherically surfaced contact lenses introduce SA in direct proportion to their sphere power (Dietze and Cox 2003). Also, human eyes have their own SA (Thibos, Hong et al, 2002). In theory, we can correct either or both of these SAs by creating a precise, radially symmetric asphericity in the lens refracting surface. One purpose of our study was to use wavefront aberrometry to evaluate the ability of clinically available aspheric lenses to correct SA.
Several anecdotal clinical accounts also exist of aspheric lenses "masking" low to moderate amounts of corneal astigmatism (Patel et al, 2004). Such masking of astigmatism is optically possible (yet unlikely) only if the lens doesn't completely conform to the corneal surface and creates a tear lens, similar to a GP lens. Using the same aberrometry technology, we also examined the ability of aspherics to correct low levels of astigmatism.
|
|
|
|
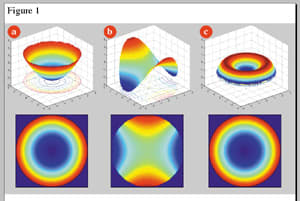
Figure 1. Wavefront error maps of a) myopic spherical
defocus. b) WTR astigmatism and c) spherical aberration. |
|
Study Setup
We employed a clinical Shack-Hartmann wavefront aberrometer (COAS, Wavefront Sciences) to quantify the monochromatic aberrations of the naked eye and of the eyes wearing various spherical, toric and aspheric contact lenses. We used two study groups. The first contained 14 eyes with low amounts of astigmatism (0.75 ±0.87D, five eyes with against-the-rule [ATR] astigmatism) to evaluate the impact of the lenses on masking astigmatism. The other study group consisted of 36 eyes with varying amounts of sphere power and less than 0.50D of astigmatism. On several of these eyes, we tested a range of lens powers to determine the impact of lens power on the lens SA.
Testing Aberration Correction
Assuming a completely deformable soft contact lens that molds to the corneal surface, one can calculate the aberrations of the contact lens itself by subtracting the naked eye measurements from the lens + eye measurements (Dietze and Cox 2003). We measured several lens types including soft spherical (Acuvue 2 [Vistakon], Frequency 55 [CooperVision], Biomedics 55 [Ocular Sciences, Inc./CooperVision], Focus Dailies [CIBA Vision]), aspheric (Frequency 55 [CooperVision], Choice AB [CIBA], Definitions AC [Optical Connection, Inc.], Biomedics Premier [OSI/CooperVision]), toric (Biomedics 55 [OSI/CooperVision]) and GP.
|
TABLE 1 Residual Astigmatism with CLs |
|
| LENS | ASTIGMATISM (DIOPTERS) |
| Acuvue 2 sphere | 0.63 |
| Choice AB asphere | 0.74 |
| Definitions AC asphere | 0.60 |
| Frequency 55 asphere | 0.64 |
| GP sphere | 0.67 |
| Biomedics Toric | 0.02 |
Understanding Aberrometry
Aberrometry data contain terms that may be unfamiliar to contact lens practitioners. Instead of the power maps we see in corneal topography, aberrometers typically quantify aberrations by wavefront error (WFE) maps. Figure 1 shows three such maps using two graphic styles. The top row shows a three-dimensional mesh or surface plot of the wavefronts, while the bottom row displays the more familiar two-dimensional color maps. These color maps show the "elevation" of the wavefront, coded by color. In an aberration-free (perfect) optical system, the wavefront map would be flat and only one color. Larger color changes indicate more aberrations and thus inferior optical quality. In general, warmer colors such as reds, oranges and yellows represent areas of a wavefront that are higher ("advanced") in relation to the reference surface, and cooler colors represent areas of the wavefront that are lower ("retarded") in relation to the reference surface.
|
|
|
|
Figure 2. WFE
maps show that aspheric lenses do not correct low levels
of astigmatism. |

For the familiar case of myopic spherical defocus (Figure 1a), the wavefront error is radially symmetric and it advances (becomes more positive) as it approaches the pupil margin. This wavefront is a sphere and will collapse down to a point at the eye's far point. Figure 1b shows a WFE map for with-the-rule (WTR) astigmatism (described at the circle of least confusion). In this map, the wavefront advances along one meridian and retards along the other. That is, at the circle of least confusion we have positive and negative defocus along orthogonal meridians. Figure 1c shows SA, a radially symmetric aberration associated with spherical lenses and present in all human eyes. It generates a more complicated WFE map, as do the other higher-order aberrations (Thibos, Hong et al, 2002).
Aspherics vs. Astigmatism
We measured the aberrations of the naked eyes and of eyes wearing a spherical Acuvue 2 lens, a Biomedics Toric lens, several aspheric lenses and a GP lens. The WFE maps in Figure 2 show the mean aberrations for all 14 eyes. We've removed the spherical defocus terms from the maps, assuming an accurate spherical correction. With the exception of the toric lens data, the astigmatic error (present in the uncorrected naked eye) dominates the wavefront maps in each case (compare the color maps in Figure 2 to the astigmatic map in Figure 1b). Table 1 quantifies the mean residual astigmatic refractive error for each lens. These results confirm that none of the tested aspheric lenses correct astigmatism.
Of course, as expected, the toric lens proved effective at correcting astigmatism (no visible sign of the astigmatic wavefront error in this map). This result held true both for eyes containing WTR and ATR astigmatism. These results reject the hypothesis that soft aspheric contact lenses mask astigmatism via an optical correction. It's unlikely, therefore, that reports of increased acuity with soft aspheric lenses actually result from correction of astigmatism. It seems possible, therefore, that this acuity improvement stems from a reduction of spherical aberration.
|
|
|
|
Figure 3. Only the Biomedics Premier aspheric lens effectively controls spherical aberration. |
|

Aspherics vs. Spherical Aberrations
Manufacturers can design aspheric contact lenses to correct for both the SA associated with the sphere power of the contact lens and the SA of the eye. Generally, spherically surfaced negative lenses generate negative SA, while spherically surfaced positive lenses generate positive SA in direct proportion to the sphere power. The black line (#1) in Figure 3a shows the relationship between sphere power and induced SA for spherically surfaced lenses. An aspheric contact lens designed to correct for this induced SA should have zero SA irrespective of lens power (red line [#2] in Figure 3a). Also, because the average human eye has roughly +0.10D of spherical aberration (Thibos, Hong et al, 2002), an aspheric contact lens with 0.10D of SA would correct this. Thus, an aspheric lens that corrects for both the SA induced by the lens itself and the SA of the eye should have approximately 0.10D of SA irrespective of the lens power (blue line [#3] in Figure 3a).
We examined the SA of 36 eyes wearing a variety of spherical and aspheric lenses over a wide range of sphere powers to examine if any of the aspherics effectively corrected for the lens-induced SA and/or the SA of the eye. By subtracting the WFE map of the naked eye from the maps generated with each of these lenses, we can quantify the aberrations of the lenses themselves. Lens aberration data from four spherical lenses (Figure 3b) and four aspherics (Figure 3c) appear using the same graphic format. It's clear that only one of the aspheric lenses (Biomedics Premier) effectively controls SA. The Biomedics Premier aspheric lens has a slope approximating zero (0.0014), indicating that it has corrected for the SA induced by the lens power, and it has an intercept of approximately 0.1D (0.1217D), indicating that it has corrected for the average amount of SA in human eyes.
How SA Affects Vision
It's clear that eyes fit with standard spherical contact lenses, as well as those fit with many of the aspheric lenses, will exhibit significant SA levels, but what are the visual consequences of SA? Figure 4a shows the color maps of the levels of anticipated SA in an eye wearing a spherical Acuvue 2 contact lens (6mm pupil diameter). The sign of the SA differs at each end of the range, being positive at low levels of sphere correction (dominated by the eye's positive SA) and negative at high minus powers (dominated by the negative SA of the lens). Notice that the minimal SA occurs not with a zero diopter correction, but with a 4.00D spherical lens. Such a lens has approximately the necessary amount of negative SA (0.1D) to correct the level of positive SA (+0.1D) in a typical eye. Thus, an eye wearing a spherical 4.00D lens will, on average, be free of SA.
|
|
|
|
Figure 4. Spherical aberration of CL + eye. |

When wearing an effective SA-correcting lens (such as the Biomedics Premier) that introduces no SA and corrects for the average level of the eye's SA, low levels of SA result (mean = 0.0139D), irrespective of the sphere power of the lens (Figure 4b).
Correcting SA would be irrelevant if it had little or no visual impact. We've calculated the optical degradation of 20/20 letters that the levels of SA in Figures 4a and 4b would generate. Notice that the levels of spherical aberration that high-power negative spherical lenses generate (left end of scale in Figure 4a) are sufficient to have a noticeable impact on visual quality. Similar image degradation occurs with low-power spherical lenses because of the eye's positive SA (right end of scale in Figure 4a). However, with the SA-correcting lens (Figure 4b) no image degradation occurs because of SA for any lens power.
Summing Up
Although the Biomedics Premier can effectively correct SA, the contact lens industry may have additional challenges to correct other higher-order aberrations that may also impact image quality. However, given the fact that lenses on the eye rotate and translate, an SA correction is perhaps more likely to succeed than would lenses designed to correct other higher-order aberrations. Also, because SA is often the largest higher-order aberration in many eyes, it may be the most important to correct.
In summary, we found no evidence that aspheric lenses optically correct astigmatism. Furthermore, most aspheric lenses don't seem to optically correct for the SA of the lenses or of the eye. However, one aspheric lens, the Biomedics Premier, effectively corrected for the SA that the contact lens power induces and the SA of the average human eye.
Ocular Sciences, Inc., partially funded this study.
To obtain references, please visit http://www.clspectrum.com/references.asp and click on document #113.
Dr. Kollbaum is a research associate at the Indiana University School of Optometry.
Dr. Bradley is a professor of Optometry and Vision Science at the Indiana University School of Optometry.