


dry eye dx and tx
Eyelid
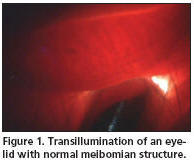
Transillumination
BY
WILLIAM TOWNSEND, OD
A frustrating facet of managing ocular surface disease is our inability to directly visualize when the glandular tissue that secretes the various components of the tears is damaged or compromised.
Imagine how a better knowledge of the true state of the diseased tissue would impact your decision making and recommendations.
Evaporative dry eye commonly results from compromised meibomian gland function. This is one area in which we can now actually evaluate the number and quality of oil-secreting glands that reside within the eyelids.
With biomicroscopy you can directly examine the yellow lines under the tarsal conjunctiva, sometimes called the piano key pattern, that are the meibomian glands. In 1982, Jester et al described the diagnostic technique of transillumination and photography of meibomian gland changes in rabbits. Robin et al (1985) showed the value of this procedure in evaluating meibomian gland dysfunction in humans.
Since
then, several studies have demonstrated the value of transillumination as a means
of determining the status of the meibo-
mian glands. Although instruments that
permit transillumination of large areas of the lids have been devised and used in
studies, none are commercially available.
Happily, virtually all eyecare practitioners already own an instrument that is useful for performing this technique: A standard transilluminator at the biomicroscope. Using it is a simple and easily mastered procedure that yields very important information about the status of these structures.

To perform transillumination, position the patient at the slit lamp in the conventional manner. Next position the transilluminator just below the lash line of the lower lid and use the instrument to evert and retroilluminate the lid (Figure 1). This allows light to pass through the lid, revealing the outlines of the meibomian glands. At this point, turn off slit lamp illumination to enhance visualization. You can see areas of partial or total loss of glandular structure using this technique (Figure 2).
Chronic inflammation and dysfunction can result in partial or total loss of meibomian glands. In most cases, dropout initially occurs in the distal portion of the gland, farthest from the orifice. Over time, tissue destruction progresses until only the proximal portion of the gland remains (proximal condensation). We find that external ocular photo-documentation (CPT-92285) is very useful in monitoring the stability or progression of this condition.
Worth the Effort
Meibomian gland transillumination is an easily mastered technique that helps to predict or explain clinical signs and symptoms. Consider adding it to your battery of tests in assessing patients who have signs and symptoms of ocular surface disease. It can help identify patients who have little potential for improvement of their meibomian gland disease because the structures are severely damaged or absent.
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #134.
Dr. Townsend is in private practice in Canyon, Texas, and is a consultant at the Amarillo VA Medical Center. E-mail him at drbill1@cox.net.