


CORRECTING ABERRATIONS
Correcting Aberrations with Contact Lenses
Part 1 of our look at the current and future realities of correcting aberrations with contact lenses.
By Pete S. Kollbaum, OD, PhD, FAAO, & Arthur Bradley, PhD

Dr. Kollbaum is a research associate at Indiana University. He can be reached at kollbaum@indiana.edu. |

Arthur Bradley is a professor of Optometry and Vision Science at Indiana University. He can be reached at bradley@indiana.edu. |
As Helmholtz once remarked, "The eye has every possible defect that can be found in an optical instrument and even some which are peculiar to itself…" The eye suffers from several types of optical defects that degrade vision, including lower-order monochromatic aberration, higher-order monochromatic aberration, chromatic aberration, distortion, diffraction, reflection, photon noise and scatter. Fortunately, some of these defects are correctable.
Following the introduction of aberrometry measurement technology to eye care over the last decade, the focus has turned to correcting not just lower-order aberrations (LOAs), but also to altering the eye's higher-order aberrations (HOAs). We've realized some progress in this area with customized refractive surgical procedures and aspheric lenses.
Smirnov, a founding father of aberration measurement, said, "It is possible to manufacture a lens compensating the wave aberration of the eye," and elaborated by stating that these lenses "must obviously be contact ones." He added, "It is unlikely that such detailed measurement will ever be adopted by the practitioner," limiting its applicability. My how times have changed! With today's aberration measurement technology it takes milliseconds instead of the 12 hours required to measure a single eye in Smirnov's time.
Today, we're witnessing a technological advancement with the potential to alter contact lens corrections. With recent advances in production technology and design, manufacturers are attempting to develop and produce lenses to correct HOAs as well as sphere power and cylinder. Additionally, this same technology is being employed to create contact lenses specifically designed to introduce additional HOAs (such as multifocals).
Characterizing Higher-Order Aberrations
Before discussing methods of correcting aberration, it's important to determine how to obtain and characterize aberration measurements. In the most common clinical aberrometers, a laser (usually of infrared wavelength) is used to create a small point of light on the retina. This point of light then becomes the source for the aberration measurements as it is reflected back through the eye's optics and out of the eye. The slopes of the exiting rays are then measured by placing a microlenslet array — an array of very small lenses (such as 0.25mm diameter) — in the exiting beam. The locations of the images created by each lenslet are directly determined by the local slope of the exiting rays. Such an instrument can quantify the ray aberrations across the pupil of the human eye (see detailed descriptions in Thibos 2000), and this design is used in the COAS aberrometer (Wavefront Sciences) that we typically use, as well as in aberrometers manufactured by Zeiss, Topcon, Bausch & Lomb, etc.
Computations then convert the ray aberration map into a wavefront map where the ray aberration is equivalent to the slope of the wavefront. For example, in an emmetropic aberration-free eye, all the exiting rays would be parallel (zero slope) and the wavefront would be flat. For a myopic eye, all of the exiting rays would converge at the far point and the exiting wavefront would be a sphere with its center at the far point.
We typically define wavefronts at thousands of points across the pupil. These are difficult to analyze or compare on their own. However, we can simplify their description by fitting the data with a series of polynomials. The thousands of raw wavefront data points are replaced by a small series of coefficients describing how much of each polynomial is required to fit the wavefront.
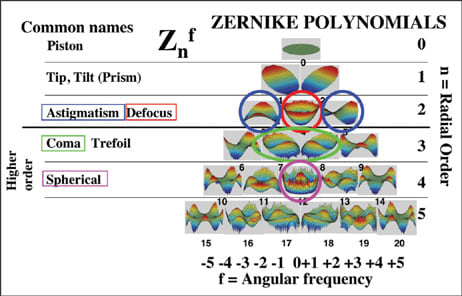
Figure 1. The Zernike "pyramid" or "tree" which serves as the road map to the Zernike polynomial expansion.
As with any polynomial fit, there will be lower-order (x1, x2) and higher-order (x3, x4) fitting terms. There are several different types of polynomials that practitioners can use, but most use Zernike polynomials. Figure 1 shows the Zernike "pyramid" or "tree," which serves as the road map to the Zernike polynomial expansion. Using the Zernike expansion to represent the wavefront error of the eye divides the eye's wavefront error into unique building blocks (astigmatism, coma, spherical aberration, etc.) that we can discuss individually.
Zernike polynomials and the pictorial representation of them in pyramid form (Figure 1) have several beneficial features. Each color map is a specific mode, or unique aberration, in the Zernike expansion. Each mode's location in the tree is designated by a radial order (n) and an angular frequency (f). When referring to a specific mode, therefore, we typically use a double index system. For example, Z4 0, spherical aberration, describes a 4th order term of 0 angular frequency.
Which Aberrations to Correct?
We often make a distinction between LOAs and HOAs. LOAs consist of the 2nd order and lower terms (such as prism, sphere, astigmatism) and the HOAs are 3rd order terms and higher in the pyramid (such as spherical aberration, coma, etc.).
Lower-order monochromatic aberrations comprise about 90 percent to 95 percent of monochromatic aberration in normal, young, healthy eyes (Porter et al, 2001; Castejon-Mochon et al, 2002; Thibos, Bradley et al, 2002; Thibos, Hong et al, 2002) and 70 percent in post-penetrating keratoplasty eyes (Castejon-Mochon et al, 2002). Even in well-focused eyes, lower-order defocus and astigmatism remain the dominant aberrations (Thibos, Bradley et al, 2002; Thibos, Hong et al, 2002).
The largest HOAs typically found in human eyes are spherical aberration and coma. Adding only these two HOAs to the LOAs represents about 99 percent of the monochromatic aberrations in normal eyes and 90 percent in the highly aberrated eyes (Castejon-Mochon et al, 2002). In young, normal eyes, the amount of higher-order monochromatic aberrations is approximately equivalent to 0.25D (Thibos, Hong et al, 2002). Although HOAs appear to be a much smaller optical problem than LOAs, vision in an eye corrected for both HOAs and LOAs will noticeably improve over that of an eye corrected only for LOAs (Yoon, 2002).
Fortunately — or unfortunately — for those desiring to optically correct HOAs, spherical aberration is the only HOA to have a population mean not equal to zero (Thibos, Bradley et al, 2002; Thibos, Hong et al, 2002). Because of this, most mass-produced contact lens corrections aimed at manipulating HOAs focus on correcting spherical aberration.
Note that current conventions for clinical description of the eye's HOAs are opposite to those for LOAs. In LOAs we describe the lens required to correct the aberration (for example, an eye with +2.00D of excess power is described as having –2.00D of myopia), whereas an eye with an excess of power at the edge of the pupil is said to have positive spherical aberration. Of course the lens required to correct for positive spherical aberration will have less power at the edge and thus negative spherical aberration.
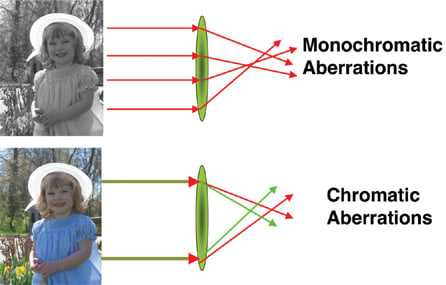
Figure 2. Monochromatic light of shorter wavelengths focuses differently than those of longer wavelengths.
Correction Challenges
There are several challenges to successful HOA correction with contact lenses. We'll concentrate on what may be perceived as the most important.
Challenge 1. As previously noted, to experience any visual gain from a correction of HOAs, you must correct LOAs to smaller levels than are currently clinically acceptable. For example, clinicians often fit a spherical equivalent sphere powered soft lens on a slightly astigmatic (<1.00D) eye. The uncorrected astigmatism may remove any benefits from correcting the much smaller coma or spherical aberration. Significant levels of uncorrected sphere (typical refraction accuracy is > ±0.25D) may also prevent any image quality gains from correcting HOAs. In younger patients we may eliminate some small spherical errors by an active accommodation mechanism. Even if we could improve refraction accuracy to less than 0.25D, manufacturers currently supply most sphere and cylinder power in increments of ±0.25D.
Several studies have determined that in the research setting we can apply HOA to lenses with reasonable accuracy (Lopez-Gil et al, 2002; Dietze and Cox, 2004; Jeong et al, 2005). It's unknown if contact lens manufacturers can yet achieve this same accuracy. Regardless, if there's any hope of experiencing gains from higher-order correction, the precision with which we measure and correct lower-order sphere and cylinder errors must improve. As clinicians, we'll have to abandon the days of leaving uncorrected sphere and astigmatism of 0.25D to 0.50D when fitting our patients.
Challenge 2. We currently perform all aberration measurements in monochromatic light (measured at one wavelength of light), which doesn't take into account that not all wavelengths of light focus at the same location inside the eye (chromatic aberration). Figure 2 shows how shorter wavelengths of monochromatic light (such as green) focus differently than those of longer wavelengths (such as red). As our world is obviously polychromatic, this difference may be critical.
Yoon et al (2002) found that correcting the monochromatic aberrations would improve acuity by about 4 logMAR acuity letters. However, correcting chromatic and monochromatic aberrations would improve acuity by approximately 10 letters (two lines). There are, therefore, two general issues that we must resolve before achieving the maximum benefits from correcting HOAs. Most aberrometers measure in the near infrared (IR) range. To correct aberrations within the visible range, you must calculate the optical errors of the eye within the visible spectrum from the IR data using chromatic aberration models or experimental data from sample eyes. Second, to gain the full benefit from correcting higher-order monochromatic aberrations, you must also correct the ocular chromatic aberrations. Currently, there is no simple way to accomplish this, although diffractive lenses may offer such an opportunity.
Challenge 3. The ability to measure aberrations and correct HOAs is limited by the accuracy of the instruments. Many aberrometers, including the one we typically use, reportedly have good accuracy (Cheng et al, 2003; Cheng et al, 2004). Additionally, the precision lathes used to create aberration-correcting lenses also are quite accurate (Lopez-Gil et al, 2002; Dietze and Cox, 2004; Jeong et al, 2005).
Challenge 4. As we all know, the eye is a dynamic biological system. Therefore, the aberrations we measure on an eye at one moment may not be the same as those we measure at another moment. This variability could result from accommodation, tears, eye or lens movements, or other unknown factors including diurnal fluctuations. This translates to a moving target for clinicians to correct (Cheng et al, 2004).
Challenge 5. The most troublesome challenge to contact lens aberration correction is that contact lenses can translate and/or rotate on the eye. Assuming a customized correction, we could account for any systematic lens positioning error (such as a lens positioned superior-nasally). These rotations and translations are less than 6 degrees rotation and 0.6mm movement with prism-ballasted lenses (Tomlinson et al, 1994). Sabesan et al (2007) found slightly smaller decentration results with their prism-ballasted lenses, noting a horizontal and vertical decentration of 0.26mm and 0.11mm, respectively.
Figure 3 shows the average on-eye horizontal and vertical decentration of an aspheric (non-prism-ballasted) soft contact lens design. Based on this sample, the mean decentration was 0.17mm horizontally and 0.29mm vertically, but, as reported by Sabesan et al (2007), there is considerable variation from eye to eye. However, non-systematic small translations and rotations about any resting contact lens position, such as those that occur with blinking, will also occur.
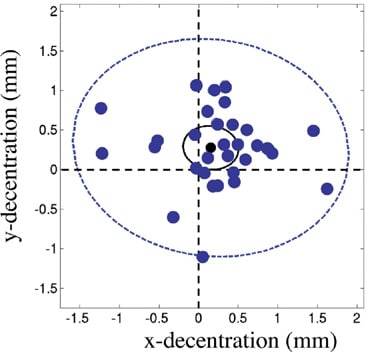
Figure 3. The average on-eye horizontal and vertical decentration of an aspheric (non-prism-ballasted) soft contact lens design.
In a few studies evaluating potential aberrationcorrecting contact lenses, the imperfect corrections attained were attributed to on-eye decentrations and rotations (Lopez-Gil et al, 2002; Dietze and Cox, 2004). Sabesan et al (2007) attempted to nullify the static lens decentration and rotation by first applying a lens blank, measuring the aberrations through this lens, and then applying the residual aberration-correction to this same type of lens.
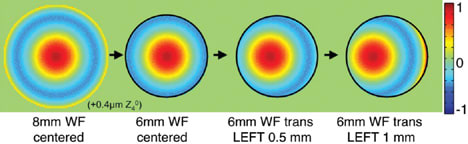
Figure 4. As the lens wavefront is decentered, the eye+lens summed wavefront has become a non-symmetric, or comatic wavefront.
Guirao et al (2001) demonstrated the impact of rotations and translations of customized corrections on image quality. They used a computational method in which they measured the wavefront of the eye, assumed an ideal correction and created a wavefront from this. They truncated this correction wavefront to a 6mm pupil diameter and then translated and rotated this correction wavefront across the eye wavefront. A similar approach is shown graphically in Figure 4. Observe that as the lens wavefront decenters, the eye+lens summed wavefront becomes a non-symmetric or comatic wavefront. Guirao et al (2001) showed that for small rotations and translations of an ideal correction, image quality remained high. However, as these rotations and translations increased, image quality approached that of a standard sphero-cylindrical correction.
Figure 5 shows the impact that translations and rotations of one mode of aberration can have on other modes of aberration. For example, in looking at rotations, we know that rotation of with-therule (WTR) cylinder correction generates against-the-rule (ATR) cylinder (circled in blue). You can generalize this to say that rotation of a particular aberration mode generates aberration of the same order (the same row of the Zernike pyramid, but the opposite side). In looking at translations, we also know that translation of sphere (circled in red) generates prism (circled in black). Additionally, translation of spherical aberration (circled in pink) generates coma (circled in green). We can generalize this result to say that a decentration of an aberration mode induces aberration of one order lower. Furthermore, the amount of this aberration induced is in direct proportion to the magnitude of aberration that was decentered and the amount of decentration (Guirao et al, 2001).
It's also important to emphasize that as a particular aberration mode is decentered, its magnitude stays the same. Again, we've experienced this clinically with decentering spherical power. Via adherence to Prentice's rule, when sphere power is decentered, prism, in known quantities, is induced (based on the sphere power and magnitude of decentration). However, as this sphere power is decentered, its magnitude remains unchanged. The same is true with decentering spherical aberration. As spherical aberration is decentered, coma is induced, but the levels of spherical aberration remain unchanged. You can see this in Figure 6 in which we systematically decentered a lens with spherical aberration and performed repeated measurements. Observe that across the range of measurements from +0.5mm to –0.5mm, spherical aberration levels remain unchanged. However, as predicted by Guirao et al (2001), with increasing levels of decentration, increasing levels of coma are introduced. In this case, as the lens was decentered horizontally, horizontal coma was introduced, but if the lens was decentered vertically, vertical coma would be introduced.
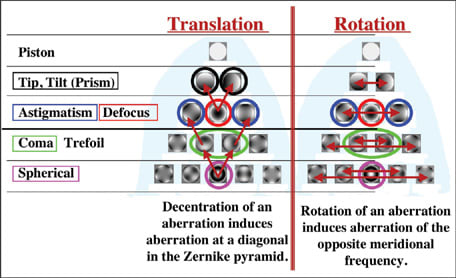
Figure 5. The impact translations and rotations of one mode of aberration have on other modes of aberration.
You can also observe in Figure 6, however, that if a lens decenters 0.5mm, an amount of coma approximately equivalent to the amount of spherical aberration is induced. If the lens is decentered 1mm, a magnitude of coma equal to twice the level of spherical aberration is induced. The lens shown has spherical aberration of about –0.21 microns. A decentration of ±0.5mm induces about 0.21 microns of coma while at 1mm, approximately 0.42 microns of coma are introduced. Thus, depending on the sign of the eye's inherent coma, typical decentration of a spherical aberration-correcting lens (about 0.5mm) could double, eliminate or change the direction and/or magnitude of the coma.

Figure 6. Horizontal coma and spherical aberration of a spherical lens with SA systematically decentered.
Guirao et al (2001) performed this same investigation on highly aberrated keratoconic (KCN) eyes. They used two approaches. In the first, they measured the aberrations of the KCN eye and then programmed them into an adaptive optics correction system (simulated KCN). In the second, they used a real KCN eye and moved it behind the measurement aperture. The results of these two methods were similar. Both methods show, with increasing lens decentrations and rotations, the ideally corrected image quality decreased toward the sphero-cylindrically corrected image quality. However, even with fairly large lens movements the benefit appears to be greater on these highly aberrated eyes than on normal eyes.
If a lens with spherical aberration levels equal to that required to correct for the population average decenters superior and nasally on the eye, it will introduce both vertical and horizontal coma. As Figure 6 shows, if a lens with 0.2 microns of spherical aberration decenters 0.5mm, 0.2 microns of coma is introduced. Therefore, if spherical aberration and coma were to have an equal impact on vision, any benefit realized by correcting spherical aberration would be lost by introducing coma. Furthermore, recent research has suggested that coma is, in fact, more visually devastating than spherical aberration by a factor of 2 (Bradley et al, 2007), meaning that a lens with spherical aberration could decenter less than 0.25mm before nullifying the benefit of a spherical aberration correction.
These results emphasize that the future success of aberration-correcting lenses may necessitate design platforms that can center well or decenter by a fixed amount. It's also worth noting that because typical spherical contact lenses exhibit spherical aberration, lens decentration-induced coma is routinely present in today's contact lens wearing population.
Challenge 6. As a contact lens conforms to the corneal surface, in most cases it will experience some shape change. The lens optics may change due to relative bending of the anterior and posterior lens surfaces when on the eye. This has traditionally been called a lens flexure effect (Holden et al, 1976). The other concern is that in addition to flexure, the lens may not completely conform to the corneal surface so an optically powered tear layer may form. This has traditionally been referred to as a supplemental power effect (Sarver 1974).
Lopez-Gil et al (2002) claimed that soft lens flexure plays only a minor role in inducing optical aberrations given a perfect match to the cornea. However, on-eye soft lens flexure may contribute to the optics of the eye+lens system if there's an imperfect match between the native topography of the lens posterior surface and the corneal anterior surface. Studies have demonstrated that particularly for higher-powered plus lenses, the on-eye power of the lens may be up to several diopters different than expected. These differences are attributed to lens flexure.
It seems possible that these flexure effects may also impact the HOAs of the eye+lens system. Ho (2003) used a series of simplistic models to estimate the optical impact of a post-lens tear layer and concluded that, although the post-lens tear layer can introduce discernable amounts of optical degradation to an ideal correction, this effect was thought to be small. However, it appears with today's on- and offeye aberration measurement technology, actual lens measurements could provide a more exact estimation of this impact. Lopez-Gil et al (2002) performed this evaluation using an interferometer for the off-eye contact lens measurements and a Shack-Hartmann aberrometer for the on-eye measurements. They concluded that on- and off-eye measurements are similar and any supplemental power effects are small, except for high-powered lenses (in agreement with Sarver 1974, Holden 1976). They also concluded that on-eye lens flexure has little impact on the HOAs of the lens+eye. However, they investigated only a very small sample of lenses with moderate-tolow levels of aberration, so this result may not be of general utility.
Dietze et al (2004) compared the aberration and relative visual benefit provided by a standard soft contact lens, a spherical aberration-correcting soft contact lens and a spherical aberration-free soft contact lens. As expected, they found that the aberration-correcting lens provided the greatest correction of the eye's spherical aberration. However, they also discovered that lenses designed to be free of spherical aberration in air increased the eye+lens spherical aberration. Lopez-Gil et al (2002) reported similar results indicating that the aberration impact of a contact lens may be slightly altered once on the eye.
A Look Ahead
In this first of a two-part series we've detailed the recent advances in measuring HOAs. We've discussed the instrumentation and the quantification of these aberrations and examined some of the theoretical challenges anticipated for correcting HOAs with contact lenses. In the second part we'll examine the current status of aberration-controlling contact lenses. We'll also summarize some of the major findings from our work and others in the field, and examine the pros and cons associated with different strategies for correcting aberrations. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #144.