


GP insights
Defining the Perfect Fit
BY BRAD GIEDD, OD, MS, FAAO
I believe one characteristic that sets contact lens specialists apart from other eyecare practitioners is that true specialists neither avoid nor decline the challenge of fitting the most difficult patients. I've also found that such practitioners tend to have a perfectionist demeanor.
One of the hardest things for these particular professionals to come to grips with, then, is the fact that managing difficult cases is not always about getting the ‘perfect’ contact lens fit. Sometimes what you might consider the most perfectly fit contact lenses are simply not acceptable to a critical patient. Conversely, a lens fit that you'd be embarrassed to present to a student may ultimately provide the best possible result for the patient.
I recently saw patients at both ends of this spectrum.
Case 1
My first patient was a 58-year-old accountant who presented with a history of GP multifocal wear. He complained that his current lenses never really provided the near acuity he needed to perform his daily work without resorting to reading glasses over the lenses. He also complained of diplopia-like shadows and end-of-day dryness. My first impression was that I could help this patient with an alternate lens design to better meet his visual needs.
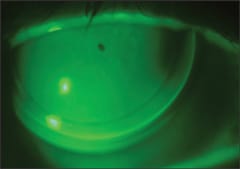
Figure 1. This GP lens fit well, but couldn't provide adequate vision.
As the examination proceeded, however, the case became a bit trickier. Corneal cylinder measured 4.00D and was complicated with a finding of a 4-prism-diopter vertical deviation. In addition, the patient's current lenses tended to strongly interact with the upper eyelid, meaning a segmented design would be difficult.
The Blanchard Evolution in FLOSI (Lagado Corp.) material provided just about every requirement (including 2 pd prism). After a few small changes to fine tune the visual acuity to 20/25+ distance and 20/30 near (with +3.00D add) and with the fit as good as I could have hoped for (Figure 1), I was satisfied. One problem, the patient was not. He required better than average near vision for doing his work, so we settled on distance-only lenses and over-spectacles for near.
Case 2
On the other end of the spectrum was a patient who presented with the most challenging post-RK corneas I've ever seen. Figure 2 shows the better right eye; the left eye had no less than 20 densely scarred incisions and developed hydrops that required penetrating keratoplasty shortly after his fitting visit.
For the right eye, we achieved success with a reverse geometry lens design that provided 20/25 acuity on this severely distorted cornea that had nearly 9.00D of irregular corneal astigmatism centrally. I wasn't satisfied with the fit — in fact, I had a hard time letting the patient leave with the lens. But there was tear exchange and the patient was comfortable with good visual acuity. He was satisfied with the lens.

Figure 2. This sub-optimal-looking fit provided good vision and comfort.
Let Your Patients Decide
In searching for the holy grail of contact lens fitting, we sometimes need to be reminded that contact lens fitting perfection is really defined as a fit that is optimal in its physiology, visual acuity and functionality for the patient. CLS
Dr. Giedd entered private practice with the Eye Associates of Winter Park in 2000, where he specializes in fitting specialty contact lenses and also performs contact lens-related clinical research.