


Online Photo Diagnosis
By William Townsend, OD, FAAO
This 56-year-old male underwent emergency retinal detachment surgery with pars plana vitrectomy and pneumatic retinopexy. Over time, the air bubble in the vitreous chamber was reabsorbed. In this photograph, the reflection of the optic nerve and posterior pole are plainly visible on the surface of the gas bubble. Selection of a gas for introduction depends on the length of time the surgeon wants the gas to reside in the eye. Sterile air is non-expansile and typically lasts approximately one week. Both sulfur hexafluoride (SF6) and perfluoropropene (C3F8) expand when injected into the vitreous. The former remains in the eye for approximately 14 days, while C3F8 resides in the eye for up to 10 weeks.
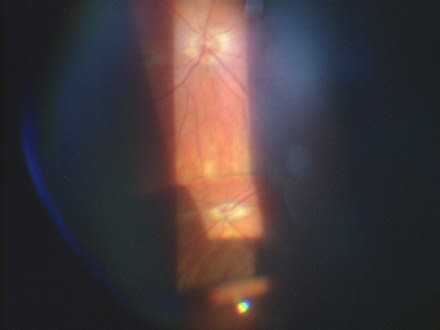
Photo credit Courtesy by Kevin Appel, OD.
As noted earlier, SF6 or C3F8 expand when introduced into the vitreous cavity, which may produce anterior displacement of the lens-iris diaphragm. This sometimes results in secondary angle-closure glaucoma with or without pupillary block. If a patient with one of these expansile gases travels from lower to higher altitude, the reduction in ambient air allows the gas to further expand, thereby increasing intraocular pressure. The rapid change in air pressure accompanying flying can cause intraocular pressures to increase up to 103 percent. Patients who have undergone retinal surgery with injection of SF6 or C3F8 should be monitored closely for IOP elevation. Appropriate management is through use of agents that reduce aqueous formation, such as topical beta blockers, carbonic anhydrase inhibitors and alpha adrenergic agonists. Avoid miotics and prostaglandin analogs in this situation. Patients whose pressures fail to adequately respond to medical therapy may require surgical intervention.