


IRREGULAR CORNEAS
A New Option for Fitting Irregular Corneas
A new large-diameter GP lens offers numerous fitting options for managing challenging irregular corneas.
By Dianne Anderson, OD, FAAO

|
| Dr. Anderson is a graduate of Indiana University School of Optometry. She practices in the western suburbs of Chicago, specializing in orthokeratology, keratoconus and post-surgical lens fits and anterior segment disease. She may be reached at Dianne.Anderson@comcast.net. |
The Rose K2 IC (Blanchard Contact Lens) is a large-diameter GP lens with a posterior aspheric optic zone. The large diameter helps provide better centration and comfort. Larger posterior optical zones help reduce flare and glare.
The asphericity of the posterior (back surface) optic zone of the lens changes as the base curve steepens. Steeper base curves require more asphericity to create an optimal lens-to-cornea fitting relationship. A sophisticated computer module adjusts the base curve to preserve the sagittal height. This adjustment depends upon base curve, power, center thickness, refractive index of the lens material and edge lift.
Fitting Approach
The Rose K2 IC diagnostic set consists of 14 lenses featuring a standard 11.2mm diameter and base curves in 1.00D increments from 6.50mm to 8.60mm. However, the Rose K2 IC is available in base curves ranging from 5.70mm to 9.30mm.
Blanchard's Systematic Approach to Fitting consists of six basic steps to achieve the optimal lens fit:
- Initial base curve selection
- Central fit
- Peripheral fit
- Diameter assessment
- Power assessment
- Managing residual astigmatism
Blanchard recommends starting with a base curve 0.3mm flatter than the steepest corneal meridian. Look for apical clearance without bubbles or a light feather touch. Once you achieve a good central fit, assess the edge lift.
Edge lift options include:
- Flat options (increased edge lift) — decreases overall sagittal height.
- Steep options (decreased edge lift) — increases overall sagittal height.
All Rose K lenses are manufactured utilizing software that adjusts the base curve, power, center thickness and paracentral fitting curves whenever a change is made to the lens periphery. This compensation preserves the optimum posterior lens touch (sagittal height) when a change in edge lift is specified. If you specify the flat edge option, the base curve will be steepened. Likewise, if you specify the steep edge option, the base curve will be flattened.
In lenses that have flatter base curves, the software automatically designs reverse geometry fitting curves — flatter central base curves with steeper alignment curves. Reverse geometry is applied to help improve fit and comfort in oblate corneas such as post-penetrating keratoplasty, post-radial keratotomy, post-LASIK and pellucid marginal degeneration.
Advanced fitting options include toric peripheral curves; front toric, back toric and bitoric designs; and Asymmetric Corneal Technology (ACT). The computer module does not automatically design these advanced options, so you must specify them. ACT can be specified to compensate for significant edge stand off at the inferior quadrant only.
I believe this simplified approach to fitting increases the probability of success, reduces the chair time required to fit these difficult corneas and provides patients an overall enhanced fitting experience with superior performance.
Rose K2 IC Fitting Options
The following case examples illustrate different fitting options available with the Rose K2 IC lens.
Case 1: Diameter and Edge Modification A 23-year-old female presented with moderate keratoconus OD and a significant nipple cone OS (Figures 1a and 1b). Her best-corrected visual acuity with spectacles is OD –6.50 –2.25 x020 20/25, OS –8.00 –2.50 x167 20/40.
I determined the following Rose K2 IC diagnostic lenses using the Systematic Approach guidelines as follows:
Steep K OD = 49.30D/6.84mm + 0.3mm = 7.14mm
Steep K OS = 50.25D/6.72mm + 0.3mm = 7.02mm
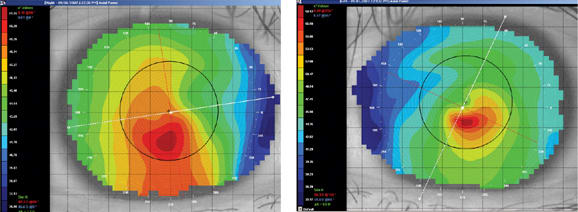
Figure 1a and 1b. Case 1 topography maps OD (left) and OS (right).
The diagnostic lenses had base curves of 7.18mm OD and 7.03mm OS. Both diagnostic lenses resulted in a good central fit, but there was a superior bubble OS as well as a tight edge at 3 o'clock and 9 o'clock OU. The 11.2mm lenses were too large for this patient's corneal diameter of 11.5mm.
Over-refraction OD resulted in plano 20/20-2 over a Rose K2 IC lens with 7.18mm base curve, 11.2mm diameter, –6.00D and OS resulted in –0.50 20/25 over a Rose K2 IC lens with 7.03mm base curve, 11.2mm diameter, –7.00D.
I decreased the diameter from 11.2mm to 9.6mm and ordered a flat (increased) edge to loosen the fit at 3 o'clock and 9 o'clock (Figure 2).

Figure 2. Case 1 custom Rose K2 IC OD (left) and diagnostic Rose K2 IC OS (right).
The final custom lenses were OD 7.12mm base curve, 9.6mm diameter, –6.50D in Boston XO (Bausch & Lomb) with a flat edge and OS 6.96mm base curve, 9.6mm diameter, –8.00D in Boston XO with a flat edge. Note how the base curve was steepened and the minus power increased to account for the flat edge.
Case 2: Back Toric Option A 26-year-old male presented with severe with-the-rule apical astigmatism. BCVA with spectacles is OD +1.00 –4.50 x005 20/70, OS –0.50 –5.50 x003 20/80.
I determined the Rose K2 IC diagnostic lenses via simulated fluorescein patterns using the Rose K2 IC designer on the Medmont (Precision Technology Services, Ltd.) topographer contact lens module. I try to create a tear film clearance of 20 microns to 35 microns (Figure 3).
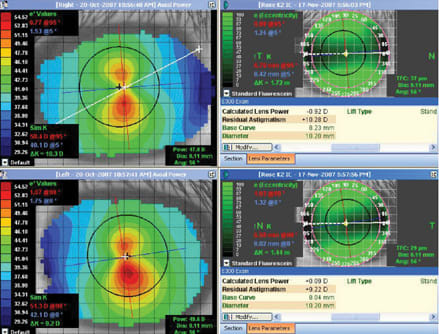
Figure 3. Case 2 topography maps and simulated fluorescein images OD and OS.
For this case the resultant base curves were 8.23mm OD and 8.04mm OS. Figures 4a and 4b show these diagnostic lenses on-eye. The edges are tight at 3 o'clock and 9 o'clock with the 11.2mm diameter, and a slight dumbbell staining pattern is visible in the horizontal meridian. Over-refraction OD was +1.50 –1.25 x005 20/30 over a Rose K2 IC diagnostic lens with 8.23mm base curve, 11.2mm diameter, –1.00D and OS was plano –1.50 x177 20/30 over a Rose K2 IC diagnostic lens with 8.04mm base curve, 11.2mm diameter, –1.00D.
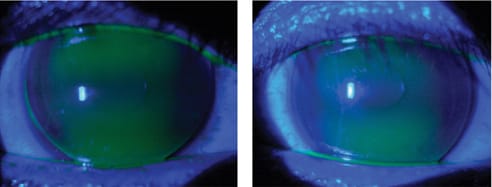
Figure 4a and 4b. Case 2 diagnostic Rose K2 IC OD (8.23mm base curve, 11.2mm diameter, left) and OS (8.04mm base curve, 11.2mm diameter, right).
I ordered back toric lenses in the following parameters: OD 8.29mm/7.34mm base curve, 10.2mm diameter, +0.50D in Boston XO with a standard edge lift and OS 8.04mm/7.18mm base curve, 10.2mm diameter, –1.00D in Boston XO with a standard edge lift.
I made no modifications to the edge as the back toric surface should loosen the fit at 3 o'clock and 9 o'clock. Figures 5a and 5b show these custom toric contact lenses on-eye. The lenses still demonstrate a slight dumbbell staining pattern with a much better edge profile because of the smaller diameter.
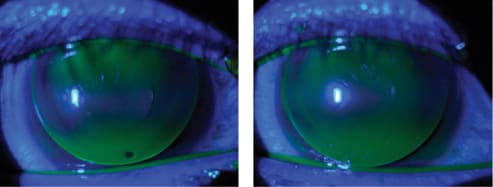
Figure 5a and 5b. Case 2 custom back toric Rose K2 IC OD (left) and OS (right).
Case 3: ACT A 38-year-old male presented with longstanding oval keratoconus and contact lens discomfort OS because of pronounced inferior edge lift (Figures 6a and 6b). BCVA in spectacles is OD –2.25 –3.25 x065 20/30-2 and OS –6.00 –2.75 x145 20/80+2
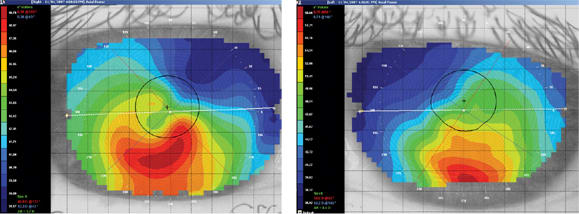
Figure 6a and 6b. Case 3 topography maps OD (left) and OS (right).
Using the Rose K2 IC designer in the Medmont contact lens module, I determined the closest diagnostic lenses. Over-refraction OD was –2.25D 20/25-2 over a Rose K2 IC diagnostic lens with 7.85mm base curve, 11.2mm diameter, –2.00D and OS was –2.00D 20/30+2 over a Rose K2 IC diagnostic lens with 7.34mm base curve, 11.2mm diameter, –5.00D. Figures 7a and 7b show the on-eye appearance of these diagnostic lenses. As you can see, the OS lens resulted in excessive edge lift at 6 o'clock, so I ordered the OS lens with grade 2 ACT.
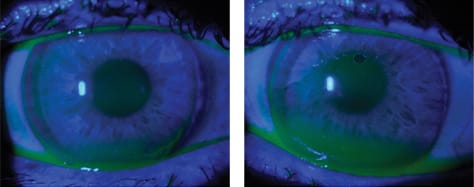
Figure 7a and 7b. Case 3 diagnostic Rose K2 IC OD (7.85mm base curve, 11.2mm diameter, left) and OS (7.34mm base curve, 11.2mm diameter).
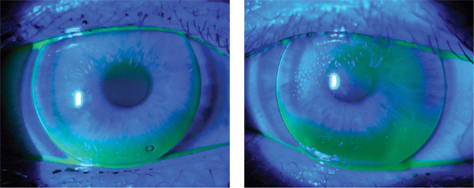
Figure 8a and 8b. Case 3 Rose K2 IC OD (left) and OS with grade 2 ACT.
The final custom lenses were OD 7.85mm base curve, 10.2mm diameter, –4.25D in Boston XO2 (B&L) with a standard edge, which resulted in 20/25 visual acuity and OS 7.34mm base curve, 10.2mm diameter, –7.00D in Boston XO2 with a standard edge and grade 2 ACT, which resulted in 20/25 visual acuity. Figures 8a and 8b show these custom lenses on-eye. The dimple bubbles subsided after an hour or so of wear. Using ACT made an excellent improvement in comfort to the OS lens.
Many Options for Irregular Corneas
The Rose K2 IC is a unique lens for unique corneas. The simplified fitting approach and numerous parameter and fitting options will help you comfortably fit your irregular cornea patients. CLS