


SOFT MULTIFOCALS
Presbyopic Soft Lens Design Options
Educate yourself — and your patients — about the benefits of multifocal contact lenses.
By Kathryn Richdale, OD, MS, FAAO

|
Dr. Richdale is a senior research associate and clinical attending in the Contact Lens Service at The Ohio State University College of Optometry. Her research is primarily accommodation and presbyopia. |
The baby boom generation, encompassing more than 76 million Americans, is now dealing with presbyopia. Survey results show that new presbyopes want to continue to look and feel young and retain their active lifestyles. Presbyopic patients cite problems with neck strain caused by using bifocal glasses. They are frustrated with reading glasses and want to remain in contact lenses. A study conducted at The Ohio State University College of Optometry gave patients who had no prior experience with multifocal or monovision contact lenses an opportunity to try each modality for one month. After trying both options, 76 percent of the patients preferred multifocal contact lenses (Richdale et al, 2006).
Despite the huge potential for presbyopic contact lens wearers, industry reports show that less than 3 percent of presbyopes are currently wearing multifocal lenses. A major reason for this disparity is that practitioners are not educating patients about all of their contact lens options and about the benefits of multifocal contact lenses. A survey conducted by the Contact Lens Council found that 40 percent of consumers did not know that multifocal contact lenses were available to correct near vision problems due to presbyopia. Research by Harris et al (2005) showed that more than 50 percent of practitioners stated that they either didn't fit multifocal contact lenses or primarily fit monovision or distance contact lenses.
Both research and clinical experience demonstrate that patients want multifocal contact lenses. We owe it to our profession and to our patients to continue to learn and improve our multifocal contact lens knowledge and fitting skills.
Improving Success with Multifocals
It's critical to start the fitting process with a careful refraction. While ±0.25D doesn't make much of a difference for non-presbyopic patients, it can have a significant impact on vision and satisfaction with multifocal lenses.
After determining the refraction, apply the correction for vertex distance and select the spherical equivalent for the initial distance contact lens power. Use a toric multifocal if the cylinder power is more than 1.00D. Again, uncorrected astigmatism may be acceptable in younger patients, but it can create too much visual compromise with a multifocal lens.
Determine the add requirements with binocular cross-cylinder testing, NRA/PRA, age, etc. It's important to determine eye dominance for every patient. Few patients are in a true balanced multifocal; it's the combination of monovision and multifocal fitting philosophies that provide the most success. To check for dominance, make sure patients are wearing their full distance correction and use a sighting method or the plus lens test.
If more than one base curve is available, begin with the steeper base curve, as decentration and excess movement are detrimental to vision quality and stability with multifocal lenses. Allow lenses to settle for a few minutes before checking fit and vision. If the fit is acceptable, check vision binocularly at distance and near. Complete all vision testing with normal room illumination. Testing under inadequate lighting conditions will give patients a negative first impression.
Always over-refract in free space with hand-held trial lenses. Putting the patient behind a phoropter creates an artificial near accommodative response and alters pupil size. When assessing near vision, use a reading card with sentences in different fonts and sizes, not individual letters.
A final key to successful fitting is patient education. Manage your patients' initial expectations by informing them that neither glasses nor contact lenses are perfect for every situation, and that it's the combination of the two modalities that provide the greatest overall satisfaction. It's important to explain how the multifocal works and that vision quality depends on pupil size and working distance. Instruct patients to add direct lighting for near work and to adjust working distance to obtain the best vision. Inform patients that there is a normal adaptation period and that knowing vision requirements for their specific work and leisure environments is critical to finding the best prescription. The fitting process improves when patients take an active role and feel that it's a joint effort to determine the best prescription for their visual needs.
Understanding Your Options
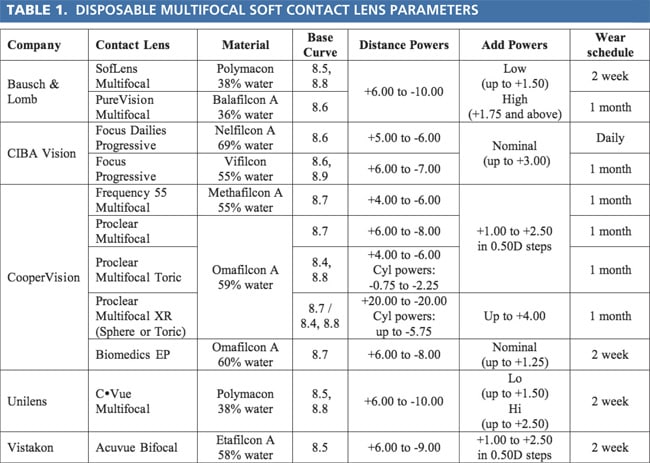
Much has changed in the world of presbyopic contact lens correction in the past five-to-10 years. There are now more than a dozen disposable soft multifocal options to meet the needs of nearly every patient. Below is a discussion of some of the many designs available. Each design has benefits, and familiarizing yourself with their differences can help improve fitting success. Tables 1 and 2 summarize the fitting parameters and designs of the soft multifocals discussed below.
Disposable Lens Options
Bausch & Lomb's SofLens and PureVision and Unilens' C•Vue multifocals are aspheric lenses with a center-near design. With either a low-add or highadd power option, they're a quick and easy-to-fit option. The basic fitting philosophy is as follows: for up to +1.50D spectacle add power, use a low-add lens OU; for an add in the range of +1.75D to +2.25D, use a low-add lens on the dominant eye and a highadd lens on the non-dominant eye; for an add of +2.50D or higher, use a high-add contact lens OU. As with most aspheric multifocals, increasing the near add power greatly effects the area of the pupil covered by the near segment. Using a high-add lens OU may compromise distance vision too much. Modifying the basic fitting philosophy by using mixed add powers and adding +0.50D to +0.75D to the distance prescription in the non-dominant eye may be a good alternative if patients aren't satisfied with their near vision.
PureVision is currently the only multifocal available in a silicone hydrogel material. It's approved for up to 30 days of continuous wear and is a great option for presbyopic patients who want continuous or flexible wear. Because of the higher modulus, it's also useful for new lens wearers or for patients who may have a difficult time handling contact lenses. Although the SofLens and C•Vue are manufactured in a lower-Dk material, they provide a less expensive option for patients concerned about cost. The lowwater content material can also help to alleviate dry eye symptoms, common in presbyopic women.
The CIBA Vision Focus Progressives lenses also feature a center-near aspheric design but have a nominal add. The lenses create an add power of up to +3.00D and are labeled with only one power that combines the distance and near prescriptions. CIBA's fitting instructions are to combine the full distance prescription with half the spectacle add (a –4.00D myope with a +2.00D add would require a –3.00D contact lens). Currently, this is the only multifocal available as a daily disposable and can be helpful for patients who have allergies or for patients who simply desire occasional contact lens wear.
CooperVision offers the most options for the presbyopic population including a toric multifocal and an extended range of distance and near powers. Their lenses offer a wide variety of options and allow subtle changes for more demanding patients or for those who have specific visual needs.
The Frequency 55 and Proclear multifocals are identical in design and combine aspheric and spherical optics in a "D" lens with a center-distance design and an "N" lens with a center-near design. The lenses have a 3mm spherical center portion surrounded by an aspheric intermediate zone and another spherical zone in the periphery.
CooperVision's fitting guidelines are straightforward and base the initial lens powers on the spectacle prescription, with a "D" lens on the dominant eye and an "N" lens on the non-dominant. You can also fit patients with a modified version of CooperVision's fitting philosophy by placing a slightly higher add power in the non-dominant eye and a lower add power in the dominant eye. For example, if a patient's spectacle add was +1.75D, begin with +1.50D "D" lens and a +2.00D "N" lens. This tends to create an appropriate balance of distance, intermediate, and near vision. For early presbyopes or for those who are dissatisfied with their distance vision in centernear aspheric designs, using two "D" lenses is a good option.
Until recently, patients who have high prescriptions or large amounts of astigmatism had to be fitted in traditional soft contact lenses or GP lenses. With the release of the Proclear toric multifocal and extended range (XR) lenses, nearly every presbyopic patient can be fitted in a disposable soft multifocal. Recognizing the importance of an accurate cylinder correction, CooperVision made the Proclear toric multifocal available in 5-degree steps.
CooperVision offers another option for early presbyopes, the Biomedics EP (early presbyope). This lens is an aspheric, center-near design similar to the "D" lens of the Proclear and Frequency 55 multifocals. The lenses are fitted with just the required distance power and provide a nominal add of about +0.75D to +1.25D. Both the Proclear multifocal and Biomedics EP lenses are manufactured in omafilcon A, an excellent material for dry eye patients.
The Acuvue Bifocal (Vistakon) is a concentric ring design with a distance center. Vistakon recommends selecting near correction based on the patient's age. This lens is a true bifocal and may challenge the demands of a more mature presbyope, but it's a wonderful choice for early presbyopes, as it's less likely to compromise distance vision than would an aspheric design. For that same reason, it also works well for emmetropes.
Conventional Replacement Options
Although more frequent disposal options are generally preferred, traditional lenses do offer some options not available in a disposable modality, or may serve as a less expensive alternative to disposables.
CooperVision, CIBA Vision and Unilens complement their disposable line of multifocals with extended parameter ranges in conventional replacement lenses. The Ultravue line of lenses (CooperVision) are the same design as its disposable multifocal and toric multifocal, but provide cylinder powers in 1-degree steps and adds up to +4.00D. The CIBASoft Progressive incorporates the same nominal add design, but is available in an expanded range of distance parameters and a toric options. The C•Vue 55 Multifocal and Toric Multifocal lenses (Unilens) also provide a wide range of parameters with cylinder axes in 1-degree steps and adds up to +3.00D.
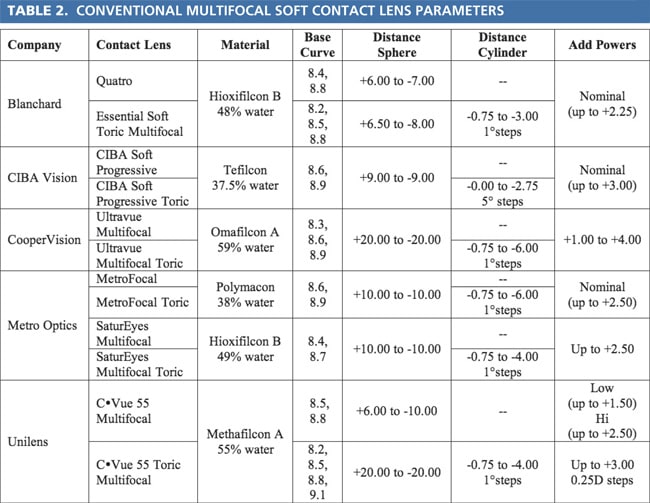
Blanchard offers a traditional soft multifocal, the Quattro lens, based on the S-form technology of its well-known GP Essential multifocal. The Quattro is a front-surface aspheric with a center-near design and is similar to the GP "Series II" design with a nominal add of up to +2.25D. Unlike other soft toric multifocals, Blanchard's Essential Soft Toric Multifocal is a double slab off design, which may improve comfort issues with high-powered prescriptions. The Essential Soft Toric is also available in a wide range of parameters with cylinder powers in 1-degree steps.
The MetroFocal from Metro Optics is a center-distance aspheric lens with a nominal add of up to +2.50D. The lens is also available in a toric design with a large range of powers and a cylinder correction at any axis. Metro Optics recently expanded the SaturEyes soft lens line to include SaturEyes Multifocal and SaturEyes Multifocal Toric lenses. The SaturEyes Multifocal and Multifocal Toric offer add powers up to +2.50D.
The Triton lens from Gelflex is the only soft translating bifocal now available. The company has a fitting guide on its Web site (www.gelflex.com).
On the horizon are the Intelliwave soft multifocal and multifocal toric contact lenses from Art Optical.
Although far from an exhaustive list of soft multifocal options, the disposable and conventional soft multifocals discussed here demonstrate the availability of parameters to fit nearly every presbyopic patient.
Final Tips for Multifocal Success
It's important to be prepared when a patient reports problems at the follow-up visit. Remember that, while patients may easily read the 20/20 line in the office, it's likely they are having difficulty during low light or low contrast conditions. It's important to listen to your patients' specific visual complaints. If a patient states that all distances are blurry or unacceptable, it's a good idea to switch to a different design — for example, change from an aspheric to a concentric ring. However, if one distance is primarily troublesome, begin by over-refracting the patient to refine the prescription.
Perform an over-refraction over the dominant eye for problems with distance vision or over the nondominant eye for near complaints. Unlike spherical or toric lenses, small changes in the distance lens power of multifocal lenses can have a profound effect on patient satisfaction. Generally, begin by adding –0.25D or –0.50D to the dominant eye for distance complaints and +0.25D or +0.50D to the non-dominant eye for poor near vision. If that change is inadequate, modify the add power. The impact of all changes should be confirmed binocularly at distance and near. Avoid making more than two to three prescription changes on one lens design. If vision isn't satisfactory, change to a different soft multifocal design or consider a GP lens.
The more familiar you become with design and fitting options the greater your success. As with most things in life, attitude is important. Being motivated and proactive in fitting multifocal contact lenses will lead to a successful and profitable practice. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #148.