


dry eye dx and tx
Recognizing Acquired Punctal or Canalicular Stenosis
BY KATHERINE M. MASTROTA, MS, OD, FAAO
Patients who have ocular surface disease frequently complain of "teary" eyes. Reflex tearing or disruption of the lipid layer often causes this symptom. However, as epiphora results from a disruption in the balance between tear production and drainage, we must also consider punctal/canalicular stenosis or obstruction.
Punctal Appearance
Punctal stenosis can be congenital or acquired. The punctal orifice is approximately 0.3mm in diameter (Figure 1). Located on the medial aspect of the upper and lower eyelid margins, each punctum sits on top of an elevated mound known as the papilla lacrimalis. The punctum are relatively avascular compared to the surrounding tissue, giving them a pale appearance that is accentuated with lateral traction of the lid. This pallor can be helpful in localizing a stenosed punctum.
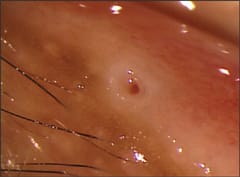
Figure 1. The punctal orifice.
Punctal Stenosis Etiology
In addition to involutional aging changes, there are numerous infectious, inflammatory, neoplastic, traumatic, and mechanical processes that can result in narrowing or occlusion of the external punctum, often with an associated canalicular stenosis.
Post-inflammatory changes from bacterial or viral infection can result in external punctal stenosis; adherence of inflammatory membranes to the punctum and canaliculus are thought to cause pathway obstruction.
Similarly, chronic blepharitis predisposes the external punctum to stenosis because of inflammatory and cicatricial changes. Chronic inflammation results in inflammatory membrane formation, conjunctival epithelial ingrowth, and keratinization of the walls of the punctum.
Ectropion has been associated with acquired punctal stenosis and canalicular obstruction, as have neoplasms, which can arise anywhere along the lacrimal drainage system.
Topical ophthalmic medications are a common cause of iatrogenic punctal and canalicular scarring; radiotherapy of the medial canthal area, graft-vs.-host disease, and cicatrizing diseases of the conjunctiva may occlude the puncta and canaliculi. Cicatrizing conjunctivitis can be infectious, allergic (e.g., atopic conjunctivitis, Stevens-Johnson syndrome), or autoimmune (e.g., ocular cicatricial pemphigoid, sarcoidosis, lupus, scleroderma) in nature.
Systemic chemotherapy is associated with acquired punctal and canalicular stenosis. The antimetabolite fluorouracil (5-FU), an anti-cancer drug, is also used in ophthalmic surgery, specifically to augment trabeculectomy as an anti-scarring agent. Systemically administered 5-FU has been known to occlude the puncta and the canaliculi.
A common adverse side effect of weekly docetaxel (Taxotere, Sanofi-Aventis) chemotherapy, which is prescribed for metastatic breast cancer, is fibrosis of the punctum and canalicular system. It is hypothesized that the chemotherapeutic agent is secreted in the tear film and directly affects the nasolacrimal system. It is estimated that up to 50 percent of patients on weekly docetaxel therapy have significant punctal and occasional canalicular stenosis.
In summary, it is important to evaluate the patency and position of the puncta and to recognize the factors that may affect their anatomy and function. CLS
Dr. Mastrota is a 1989 graduate of SUNY State College of Optometry. Currently she is Center Director at the New York Office of Omni Eye Services. She is also a consultant to Allergan, AMO, B&L, Inspire, and Cynacon OcuSoft.