


GP insights
20 Pearls for Managing Post-PK Patients With GP Lenses, Part 1
BY EDWARD S. BENNETT, OD, MSED, JEFFREY SONSINO, OD, & BRUCE ANDERSON, OD
Whenever we think about the adage of no two eyes being identical in the contact lens industry, postpenetrating keratoplasty (PK) patients often come to mind. With the help of some experts in the management of these patients, the next three columns are devoted to clinical pearls beneficial in fitting these patients with GP lenses.
Step 1. The first step in fitting a lens for post-PK is determining the shape of the donor tissue. Using (preferably) corneal topography, is the graft prolate (steep centrally with rapid change in eccentricity and a flat periphery), oblate (flat centrally, steepening toward the periphery), or tilted?
Step 2. If the graft is prolate, think of the shape as similar to a keratoconic eye and fit lens designs that accommodate a steep central zone. A great option on a prolate graft is an aspheric posterior surface lens, followed by keratoconic designs such as AKS (Art Optical) or Rose K (Menicon).
Step 3. If the graft is oblate, the shape is similar to a post-radial keratotomy eye. A standard diameter lens will decenter, almost like placing a plate on a table and then shaking the table. Typically, large-diameter lenses are most successful; however, it is important to avoid air bubbles at the graft-host interface (Figure 1). The reason air bubbles may be present when using a large-diameter lens is that such lenses tend to contact the host tissue, which does not continue the oblate shape of the graft. The lens will seek the steepest portion of the cornea and decenter to the steepest portion of the graft-host interface. When this occurs, a large-diameter, reverse geometry lens will often solve the problem (Figure 2).
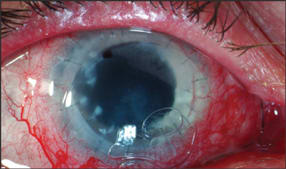
Figure 1. It is important to avoid air bubbles at the graft-host interface.

Figure 2. A large-diameter, reverse geometry lens often eliminates the bubbles.
Step 4. Tilted grafts are the most challenging of these cases. The best option is typically a bitoric design to fit the elevated portion like a lock and key.
Step 5. Think large when fitting irregular corneas, most of which are fit with GP lenses 10mm and larger. Obtain fitting sets of the intralimbal designs to try on patients. Semi-sclerals represent an additional tool to have in your post-PK tool box.
Step 6. Have the topography in front of you when looking at the patient under the slit lamp and when trying different lenses on the eye. Visualize what is measured on the topography and what you expect to see when examining the patient. How does the lens sit on the cornea, where does it touch, what do the edges of the lens look like? Do you see what you would expect based on the topography map? Being able to read the topography details will help you obtain a good fit faster and more efficiently. CLS
Dr. Bennett is an associate professor of optometry at the University of Missouri-St. Louis and is executive director of the GP Lens Institute. Dr. Sonsino is the chair of the American Optometric Association's Anterior Segment Committee and an assistant professor at Vanderbilt Eye Institute in Nashville, Tenn. He has received research funding from CIBA Vision. Dr. Anderson practices in Tampa, Fla., and is the director of the Contact Lens Clinics at the University of South Florida, College of Medicine Department of Ophthalmology.