


ORTHO-K FITTING
Reducing Chair Time With Orthokeratology
Instrument and computer technology can help you profitably incorporate orthokeratology in your practice.
By Robert W. Kirkpatrick, OD

Dr. Kirkpatrick has a private practice in primary care optometry in Madison, Indiana. He received his clinical degree in Optometry from Indiana University in 1976. He has served on the National Board of Examiners, is past president of the Indiana Optometric Alumni Association, and has been appointed by the Governor to serve as a member of the Indiana State Board. |
For a number of years, I've been following with interest the published studies and presented lectures on modern accelerated orthokeratology. I was very keen to introduce this treatment in my practice, but I wanted a method that wouldn't require hours of chair time for every patient.
When reviewing the different methods, a number of questions came to mind. What do I need to know about reverse geometry lenses? How much fluorescein analysis will I need to perform? How many patient visits are required and for what duration each time? How do I modify and problem-solve treatments? There are many published studies demonstrating that ortho-k is a safe and effective treatment. However, did I have the time to implement the treatment, achieve both expertise and proficiency, and ultimately make it a successful addition to my practice?
Finding the Right Method
For ortho-k to work in my practice, I wanted to find a system that could more heavily involve my staff rather than monopolize my chair time. Secondly, I wanted a method that could rely more heavily on technology to fit and problem-solve.
We chose the BE Retainer (BE Enterprises, Inc./Essilor) design as it relies exclusively on topography data and fitting software throughout the entire process. This allowed me to train my staff to perform 90 percent of the ortho-k fitting process without requiring me to spend lengthy office visits evaluating fluorescein patterns and troubleshooting. To coordinate this new treatment in our practice, we selected a technician to be our exclusive orthokeratology technician.
The Fitting Process
Following our usual pre-contact lens fitting assessments (patient history, eye health exam, prescription), our coordinator takes four independent corneal topography readings of each eye. The accuracy of our corneal data determines the success with the initial diagnostic lens, so our technician takes the time to achieve four quality captures OU (Figure 1). Any maps demonstrating tear film breakup, inconsistencies, small fissures or unusual appearing plots are deleted and retaken. Our office uses the Medmont E300 Corneal topographer (Medmont/Precision Technology Services, Ltd.) because we find that it is accurate and because it features software designed for orthokeratology and specialty contact lens fitting.
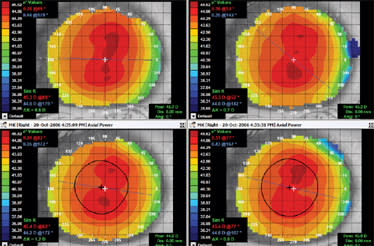
Figure 1. Baseline topographies of the right eye. Look for similarities (reproducibility) from capture to capture as a gauge of accuracy.
After confirming that we have four quality corneal topography maps that appear identical (reproducible plots), our next step is to extract the shape data from our instrument.
Only three pieces of corneal data are required from our topographer: the apical curvature or radius at the apex of the cornea (also known as Ro or Radius at zero), the sagittal height of the cornea and the horizontal visible iris diameter (HVID). From the topography captures, the software determined the mean values for the apical radius (7.511mm) and sagittal height (1559.1 microns). Figure 2 shows our measure of the HVID.
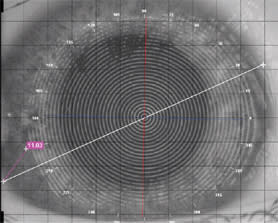
Figure 2. Measuring horizontal visible iris diameter (HVID) or corneal diameter.
Once we acquire the necessary topography data, we run our BE Retainer orthokeratology fitting software. In addition to entering a patient's spectacle prescription, we choose a treatment target typically 0.50D greater than the spherical myopic error. This is to assure that the patient's acuity is no worse than plano at the end of the day while the cornea slowly regresses following morning removal of the overnight retainers. In addition, with time the +0.50D over-correction may allow patients to have acceptable vision for several days before they need to wear their lenses again. We've found that many patients with a correction of <–2.00D need to wear their lenses only every four nights or about twice per week.
After entering the corneal data, the software determines whether the patient is a good candidate for ortho-k treatment. In this case, the calculated potential for change is –3.64D OD. On this particular eye, the software predicted that the cornea could achieve up to 3.64D of orthokeratology effect. With the software designing a lens with a smaller treatment zone, another 1.00D over and above this figure is predicted possible based on the models of corneal shape relating to ortho-k treatment. This patient has a spectacle prescription of –2.50 –0.75 × 120 (therapy target of –3.00D), so the patient is an excellent candidate because the treatment goal is much lower than the corneal potential for change (as determined by the fitting software).
If patients want to proceed with ortho-k treatment, the next step is to calculate the diagnostic parameters necessary. For our patient, the software indicated that we required an 8.25mm BE Retainer diagnostic lens. At this point we instructed the patient on the proper handling of a GP lens (Boston Equalens II material, Bausch & Lomb) and taught application and removal techniques. We scheduled the patient to wear this lens overnight for the night immediately prior to our morning evaluation.
We instruct our patients to apply their lenses immediately before sleeping and to come into the office with the lenses in situ. Having patients wear the lenses into the office can result in heightened awareness, but it's critical for a number of reasons. It allows you to observe the physiological and topographical effects immediately after removal. Any adverse events are readily apparent directly following lens removal. Additionally, after only one night of wear the corneal retention of the effect is minimal, so the clearest picture of the topographical result is best diagnosed immediately following removal.
During our morning evaluation, we first determine whether patients have the correct diagnostic lenses on the correct eyes by noting the corresponding letter engraving. Secondly, it's important to assess lens movement. Adherence is a common characteristic of ortho-k lenses and results from the changing tear film viscosity during wear. Adherence is not an adverse event, but removing an adhered lens can cause one. Therefore, it's important to educate patients on what an adhered lens looks and feels like. You must also teach patients how to safely loosen an adhered lens prior to removal, as outlined below.
If our diagnostic lens is not moving freely, we instill artificial tears, instruct patients to look up and then press with the finger into the lower lid and sclera three times with firm pressure. Patients should then look down, and we perform three similar presses into the superior lid and sclera. Determine after this procedure whether the lens is moving well. If not, repeat the steps until it is. Once the diagnostic lens is no longer adhered, we will remove it and check for staining and for any adverse physiological events. We particularly look for corneal staining and any evidence that the lens was in contact with the central epithelium.
A quick acuity evaluation precedes corneal topography. Note that we have not checked the fit of the lenses on-eye nor devoted much time performing post-treatment fluorescein pattern analysis or over-refractions. Corneal topography tells us everything we want to know about the effect of our treatment: treatment zone position and size, lens position in the closed eye environment, and the prescription change. Your technician or ortho-k coordinator can perform all of the procedures with the exception of the biomicroscopic evaluation, which usually takes only about five-to-10 minutes in the morning.
Following the slit lamp exam and acuity evaluation, corneal topography is performed. The technician takes one or two maps, then selects the subtractive map function and compares the baseline (pretreatment map) against the morning post-treatment map. The technician analyzes the subtractive map on each eye using three separate topographical interpretations:
1. Axial Subtractive Map Determines the treatment zone position (blue central area of flattening) in relation to the pupil margin (black ring). The prescription change or effect of treatment can be observed by measuring the apical power difference. The technician can determine the change in refraction by clicking the cursor on the center of the map (visual axis).
2. Tangential Subtractive Map Determines the position of the ortho-k lens in the closed eye environment. Look at the red ring of paracentral steepening in relation to the pupil margin. A well-centered lens will appear to have a red ring that runs parallel to the black pupil margin
3. Refractive Subtractive Map Determines the size of the treatment zone.
It is at this point that the technician or practitioner must determine the topographical response. Was it a perfectly centered response — a topographical bulls-eye (Figure 3)? Was it superiorly positioned — a smiley face topographical response (Figure 4)? Was it an inferiorly positioned response — a frowny face (Figure 5)? Or was there apical steepening — a central island response (Figure 6)?
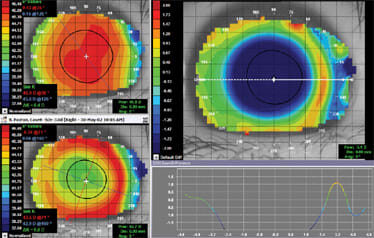
Figure 3. Bulls-eye topography — centered post-treatment subtractive map (axial map).
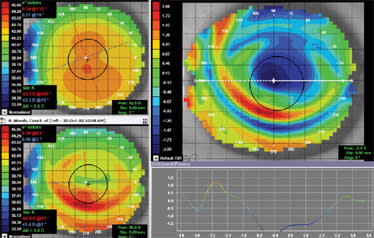
Figure 4. Smiley face topography — superior positioned post-treatment subtractive map (axial map).
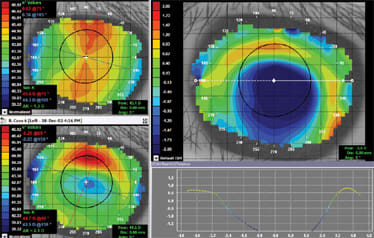
Figure 5. Frowny face topography — inferior positioned post-treatment subtractive map (axial map).
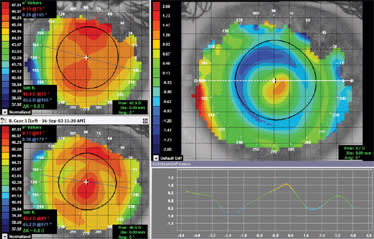
Figure 6. Central island topography — apical steepening post-treatment subtractive map (axial map).
We employ the "subtractive" or "difference" map function in our topographer to determine the response to treatment. If our office is uncertain of the response, we e-mail our consultant directly from the topographer to acquire immediate determination of the effect.
Finalizing the Fit for Our Case Example
Figure 7 shows the one-night post-treatment topography of our patient, with an acuity of 20/50. As you can see, the central cornea did not respond as significantly as did the peripheral cornea. Only a percentage of effect was achieved after one night of wear. Considering this as well as that the visual acuity was significantly improved and the treatment zone (blue area of flattening) looks well-centered, we continued the trial wear for additional nights to prove out the effect.
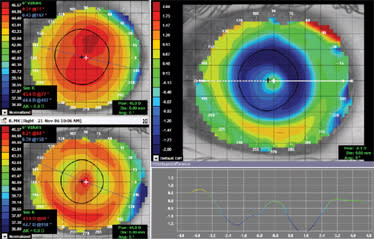
Figure 7. One-night post-treatment topographical response. Note the reduced apical effect with greater peripheral flattening (axial subtractive map).
We instructed the patient to wear the lenses only overnight for an additional four consecutive nights. The true effect of any ortho-k lens may not be definite after one night of treatment. By continuing the trial process for multiple nights, the topographical and prescription effects of the lens become absolute. This method also allows patients to experience both the treatment and the improvement in vision over the course of several days.
At this point, very little has been invested by either our practice or our patients. Only when both patient and practice are certain of the result do we incur the cost of the custom lens. Figure 8 displays the post-treatment subtractive map after five consecutive nights of wear. Note a more significant apical effect and a treatment zone that has filled in nicely. The patient's VA improved from 20/50 after one night to 20/20 after five nights.
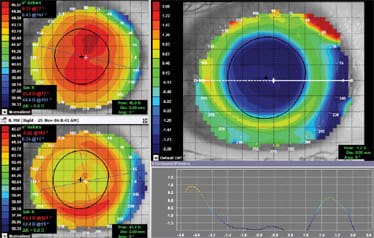
Figure 8. Post-treatment response after five nights of consecutive wear showing a well-centered bulls-eye with a –1.70D prescription change (axial subtractive map).
Once the topographical response exhibits a definite pattern, we open the fitting software again and click on the last record for our patient, which has the parameters of the current diagnostic lens. The software will then ask for the topographical response. If we enter that the topography showed a central island or smiley face, the software will select the ideal next diagnostic lens to try. The software will instruct you to allow the cornea to normalize prior to wearing the new diagnostic lens so that the immediate outcome is not affected by any adverse alteration in the shape of the cornea from the previous lens.
If the topographical response was a bulls-eye, then the fitting software will ask for the prescription change that the diagnostic lens produced (in this case it was –1.70D). It is not important that the trial produces the ideal refractive response. However, it is important that the trial produces a measured prescription change that can be used in relation to the requested target prescription. The software will calculate the ideal custom parameters from the two (comparing the actual outcome of the diagnostic fitting versus the desired target prescription). This step concludes the diagnostic process, so we allow the cornea to normalize prior to the arrival of our ordered custom BE Retainer parameters.
We require that our patients' corneas return to baseline shape prior to wearing new custom lenses. This allows us to see the immediate effect of new lens parameters on-eye to be sure the physiological and refractive goals are being achieved. While patients' eyes return to a normal shape following the diagnostic fitting, we provide soft lenses if necessary to aid vision if the diagnostic lens under-corrected vision. Typically, for every consecutive night of ortho-k wear, patients must take an equal number of nights off wear for the cornea to return to baseline.
Once the new custom BE Retainer arrives, we schedule the patient for the first overnight wear of the new custom parameters. This will be the last time the patient wears the lenses into the office. We follow the same one-night trial procedures:
Patient Instructions:
- Fill the back surface of the lenses with GP solution.
- Apply prior to sleep.
- Return to the office early in the morning for evaluation with the lenses in situ.
Morning Practice Procedures:
- Check for lens movement and free adhered lenses.
- Remove lenses.
- Check physiological response.
- Check visual acuity.
- Perform corneal topography.
The full effect of any ortho-k lens takes seven-to-10 days (Alharbi and Swarbrick, 2003). It is typical after one night for there to be an under correction. As long as the topography shows the initiation of a centered bulls-eye pattern and the physiological response looks acceptable, we schedule patients for a return visit after one week or two weeks of wear. Figure 9 displays our patient's one-night response, which provided a mild –0.50D prescription change and visual acuity of 20/15 –3.00. Because ortho-k treatment produces less than the required prescription change after only one night, we will supply soft lenses to fill in for the first day or two while the treatment increases in effect.
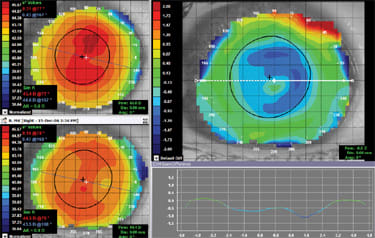
Figure 9. One-night post-treatment response in the custom lens. The beginnings of a well centered bulls-eye topography are evident (axial subtractive map).
At the one- (or two-) week visit, patients should have achieved the target prescription change wit hour initial custom order. Figure 10 shows our patient after the lens has achieved full effect at 16 days. Note the large, uniform treatment zone and higher –2.80D prescription change and visual acuity of 20/15 –1.00.
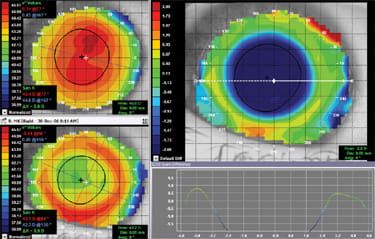
Figure 10. Bulls-eye topography after 16 nights of wear displaying a large, uniform treatment zone and –2.80D prescription change.
The next visit occurs following one month of wear. We ask patients to visit late in the afternoon. If a patient is refracting at +0.25D or +0.50D this late in the day, then we review a reduced wear schedule. Our patients become very good at determining what frequency of wear will provide ideal acuity. We then schedule patients to return every six months to monitor corneal health and ortho-k effect.
A Great Practice-Building Modality
In summary, orthokeratololgy has definitely created new income-producing and challenging opportunities for our practice. The technology is the first of its kind in our area. The community is excited about it. I think the best referrals have come from young high school athletes who are now free of corrective lenses. Many new patients visit us inquiring about the BE Retainer. Most have remained loyal patients even though many of them do not qualify for orthokeratology. CLS
Special thanks to Mary Ann Kail of Essilor Contact Lens for her assistance with training and support.
For references, please visit www.clspectrum.com/references.asp and click on document #161.