


contact lens case reports
A Closer Look at SEALs
BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRÉ, FAAO
In clinical practice, specific complications tend to appear in waves. So has been the appearance of superior epithelial arcuate lesions (SEALs), also know as epithelial splitting. In early stages SEALs are characterized by the appearance of scattered punctate dots of corneal staining aligned in an arcuate fashion running parallel to the superior limbus. In later stages staining coalesces to form a deep arcuate epithelial lesion approximately 1mm to 3mm in length between 10 o'clock and 2 o'clock. The edges of the lesion are often raised and irregular, and there is usually a 1mm zone of clear epithelium separating the lesion from the superior limbus.
A SEALs Case Study
A 24-year-old female with a 12- month history of wearing Acuvue Oasys (Vistakon) lenses for the correction of her −7.75D of myopia presented with the history of three days of mild discomfort in her right eye only. Slit lamp exam revealed a grayish-white, full-epithelial- thickness SEAL on the right eye only (Figure 1). The left eye was unremarkable. We treated the lesion by discontinuing lens wear and prescribing preservative-free artificial tears every two hours while awake.
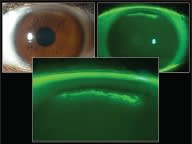
Figure 1. A SEAL on the patient's right eye.
Experience had shown us that these lesions heal within 48-to-72 hours with no residual corneal scarring. Hers followed the anticipated course and was 95 percent healed within 48 hours (Figure 2).
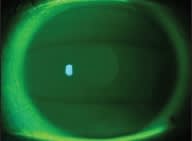
Figure 2. The SEAL 48 hours after lens discontinuation.
The mechanism(s) for this epithelial disturbance are poorly understood. However, in 1993 Young and Mirejovsky suggested the primary cause was mechanical trauma related to lenses that do not adequately align the contour of the peripheral cornea and sclera. In certain patients, lens material characteristics and/or design features can result in an excessive vaulting of the lens across the superior limbus. As the upper lid descends across the vaulted lens, it collapses against the cornea resulting in mechanical trauma and an epithelial defect.
A striking feature of SEALs is their relative asymptomatic nature despite the lesions' size and depth. This is probably related to their location in the peripheral area of the cornea and that they occur beneath the upper lid.
Factors likely to encourage SEALs include stiff, high-modules lens materials, thick lenses, dehydration, and small corneal diameters or less-than-normal sagittal heights.
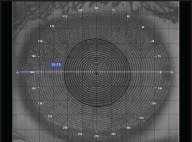
Figure 3. The patient's small HVID of 10.7mm.
Our patient had significantly smaller-than-normal corneas with HVIDs of 10.7mm (Figure 3). We suspect the lesion might have been related to excessive lens vaulting over her cornea with minimal sagittal height. We refitted her in Focus Dailies (CIBA Vision) and are monitoring her for any recurrence. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #165.
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision.