


pediatric and teen cl care
Set Realistic Expectations for Corneal Reshaping
BY MARJORIE J. RAH, OD, PHD, & JEFFREY J. WALLINE, OD, PHD
Incorporating orthokeratology or corneal reshaping into your practice can be rewarding. More than any other lens patients, these patients will serve as a referral source to friends and relatives. It is important, however, to maintain realistic expectations for outcomes of the treatment.
Patient Selection
Many lens designs are available for fitting corneal reshaping patients. The simplest systems allow you to send the keratometry readings and spectacle prescription to the lab where the first lens is designed. Others provide fitting sets for in-office diagnostic evaluation of lens fits. Dispensing sets are available for some designs, allowing lenses to be dispensed directly from the diagnostic set on the day of the fitting.
Patients with lower refractive errors are more successful compared to higher myopes. Although FDA approved for temporary myopia reduction up to −5.00D to −6.00D, data from the FDA clinical study for Vision Shaping Treatment (VST, Bausch & Lomb) and Paragon CRT (Paragon Vision Sciences) lenses show a decrease in the percentage of patients achieving full correction as initial myopia increases above −4.00D (Figure 1).
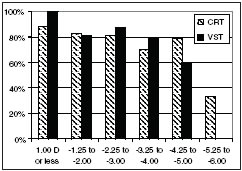
Figure 1. Percentage of patients who achieved full reduction within ±0.50D of the targeted treatment. Data obtained from package inserts.
Success will come from selecting patients who have lower amounts of myopia. However, for patients who have greater than −4.00D of myopia, education of the success rates is essential.
Set Goals Early
The current trend is for families to bring their children into an eye examination with hopes that there is an ideal solution to slow or halt myopia progression. Some believe that corneal reshaping will be the answer. When incorporating orthokeratology into your practice, this is a topic you will discuss frequently with parents and patients.
Despite positive data from recent studies by Cho et al (2005) and Walline et al (2009) (Figure 2), there are currently no guarantees that corneal reshaping will slow or halt myopia progression. It is often also necessary to remind patients and parents that corneal reshaping does not eliminate myopia permanently.
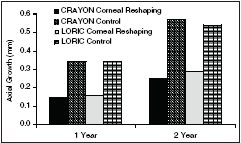
Figure 2. Mean axial growth data from years one and two of the CRAYON (Walline et al, 2009) and LORIC (Cho et al, 2005) studies comparing corneal reshaping treatment to controls.
All staff members should understand the basics of corneal reshaping to provide a consistent message. Setting realistic expectations from the start is one of the most important aspects of corneal reshaping treatment. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #165.
Dr. Rah is a staff optometrist at the Massachusetts Eye and Ear Infirmary Contact Lens Service where she specializes in medically necessary and other advanced contact lens designs. Dr. Walline is an assistant professor at The Ohio State University College of Optometry, where he conducts studies of pediatric contact lens wear. He is also a consultant or advisor and has received research funds from Paragon and Vistakon.