


SCLERAL LENS DEVELOPMENT
Evolution of an Ocular Surface Prosthesis
The development of an adaptive design process may help revolutionize scleral lens fitting
By Perry Rosenthal, MD

Dr. Rosenthal is a salaried employee and founding president of the 501(c)3 nonprofit Boston Foundation for Sight and has no proprietary interest in the Boston Ocular Surface Prosthesis. He is also an assistant clinical professor of ophthalmology at Harvard Medical School and an adjunct faculty member at the New England College of Optometry. |
In 1887, two European ophthalmologists independently inserted water-filled glass optical shells on patients' eyes, thereby fitting the first contact lenses (Fick, 1888). Although impractical, they provided proof of principal of a theory that Leonardo da Vinci implied in his Codex of the Eye (1508) that creating a smooth boundary of fluid over an irregular corneal surface could improve vision.
Early Sclerals
The introduction of plastic in the early 1930s, with its advantages of being lightweight, shatterproof, and moldable, attracted the attention of Dr. William Feinbloom, a New York optometrist who was the first to incorporate (poly)methylmethacrylate (PMMA) into a scleral lens. However, the promise of plastic was stymied by the rapid development of misty vision soon after lens application. In addition to this microcystic corneal epithelial edema (then known as Sattler's Veil), some patients who continued to wear them as their only means of achieving functional vision developed corneal neovascularization — a legacy that taints the reputation of even today's GP scleral lenses.
In 1952, Smelzer and Ozanics published a seminal paper in Science proving that the cornea, devoid of blood vessels, extracts the oxygen required for its metabolism from the tear layer. By covering the entire surface of the cornea, PMMA scleral lenses blocked the corneal oxygen supply. Sattler's Veil and corneal neovascularization were complications of corneal asphyxiation.
The Advent of Corneal Lenses
Fenestrations and slots failed to adequately mitigate early sclerals' induced corneal hypoxia. But the nail in their coffin was delivered by Kevin Touhy, a Los Angeles optician, who fortuitously discovered that in making contact lenses small enough to leave a portion of the corneal surface exposed to the ambient air, he had relegated Sattler's Veil to the dustbins of history. The longer wearing times, ease of fitting and handling, and lower cost of Touhy's lenses appealed to the American entrepreneurial spirit, and the rigid corneal contact lens based on Touhy's 1948 patent dominated the hard contact lens market for the next 60 years. The introduction of soft contact lenses in the early 1970s threatened the survival of the GP contact lens market. Although boosted by the introduction of GP polymers in the 1980s, once the captive population of PMMA corneal contact lens wearers was exhausted, GP contact lens manufacturers faced a bleak future shrinking market. The one exception was patients for whom wearing a rigid lens was the only alternative to corneal transplant surgery.
However, in exploiting this market niche, manufacturers relied on a hard lens designed to rest on and slide over the diseased cornea, a fragile tissue protected by an exquisitely sensitive alarm system of pain sensors. Not only is the density of corneal pain nerve endings estimated to be 20-to-40 times that of dental pulp (Muller et al 2003), these pain-generating nerve terminals are located just under a tenuous tear/mucin layer. Thus the wearability of corneal GP contact lenses is dependent on a robust and well lubricated corneal epithelial surface that has a smooth and appropriate shape — requisites that diseased corneas rarely meet.
That is why statistics regarding outcomes in fitting diseased corneas with corneal GP contact lenses should be qualified. "Success" is defined as the lenses being worn consistently. Tolerance is not even in the equation. In many (if not most) of these patients, their continuing to wear corneal GP contact lenses is driven by:
- The severity of spectacle-corrected visual impairment (motivation)
- The skill of the fitter in minimizing wearing discomfort and corneal erosions
- Patients' fear of the serious risks and uncertain visual outcome of corneal transplant surgery
It is an unfortunate paradox that patients who can benefit the most from the unique optical benefits of rigid lenses are the ones least able to tolerate them.
Developing a Modern GP Scleral Lens
Patients who had corneal disorders faced a bleak future when in 1983 Donald Ezekiel, an innovative optometrist in Perth, Australia, reported the first successful use of scleral lenses fabricated from a GP polymer (Boston II, Polymer Technology Corporation). Here was a way to provide the optical benefits of GP contact lenses without traumatizing diseased corneas. Yet this milestone paper stirred little interest in the eyecare professions, in part because of the lingering reputation of discredited PMMA scleral lenses. Some practitioners may also have been intimidated by the need to manage the air bubbles aspirated through fenestrations required to supplement the otherwise inadequate oxygen permeability of the early GP polymers.
In 1986, coincident with the development of Boston IV (the first of a new generation of high-oxygen flux polymers), I examined a patient whose better eye had been repaired after a traumatic rupture that left it aphakic with 12.00D of against-the-rule astigmatism. In the absence of other options for rehabilitating vision, we made the first non-fenestrated GP scleral lens using a manual lathe. The result was 20/30 vision, all-day wearing comfort and excellent corneal tolerance. I remember thinking that it couldn't be this easy.
It wasn't. Failures were common. Most resulted from excessive scleral compression that caused bul-bar conjunctival congestion and chemosis — not surprising since the entire compressive force of a scleral lens is focused on this surface (Figure 1).
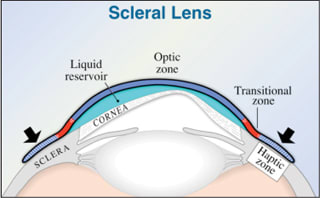
Figure 1. A standard scleral lens design tends to cause scleral compression.
Suction: The Achilles Heel of the Fluid-Ventilated Scleral Lens More serious was the development of dangerous lens suction. This results from circumferential scleral compression that blocks the ingress of tears into the fluid compartment during lens decompression, preventing replacement of the volume fluid squeezed out during each blink or ocular versions.
The need to prevent uncontrolled lens suction was paramount. The only alternative to fenestrations are channels between the bearing surface of the haptic and the underlying sclera that are large enough to accommodate the inward seepage of tears into the fluid compartment to abort the development of suction and yet small enough to prevent the transit of air bubbles. I coined the term "fluid-ventilated" for this lens to distinguish it from the air-ventilated fenestrated scleral lens design.
Through trial and error I discovered that large lenses (20.0mm to 23.0mm) consistently avoid developing excessive suction. The reason for this is that the peripheral surface of their haptic extends over the insertions of the rectus muscles. This elevates the haptic sufficiently to facilitate the transit of tears into the fluid reservoir. On the other hand, large scleral lenses are more challenging to apply, especially on more deeply inset eyes and those with smaller palpebral fissures. Moreover, the circumferential asymmetry of the globe's surface in the deep recesses of the fornices that aids tear exchange can sometimes create an air meniscus under the peripheral haptic that increases lens awareness and may facilitate the transit of air bubbles into the fluid reservoir.
Why Not Fit Small Scleral Lenses? Keep in mind that any reduction in the size of scleral lenses occurs at the expense of the haptic. It is a simple rule of physics that as the haptic bearing surface is reduced, compression becomes more narrowly focused on the scleral surface. Moreover, if the bearing surface of the haptic does not match the underlying surface of the sclera closely enough, its compressive force becomes even more concentrated on the scleral high points. The bottom line is this: the smaller the haptic surface area, the greater the scleral compression and the more important it is to align the posterior haptic surface with that of the underlying sclera. However, below a minimal diameter, even uniformly distributed scleral compression becomes intolerable.
In addition to their limited surface area and increasing scleral compression, smaller scleral lenses rest closer to the limbus where scleral surfaces become more circumferentially uniform. This increases the likelihood of circumferential scleral compression resulting in lens suction, limbal bulbar conjunctival vascular engorgement/stasis, Chemosis, and, in extreme cases, intense corneal edema. Although focal scleral compression is easily identified by zones of blanching of the underlying bulbar conjunctiva blood vessels (Figure 2), preventing or eliminating it has been far more challenging.
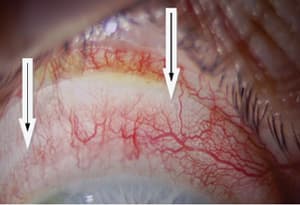
Figure 2. Arcuate zones of scleral compression at blended junctions of connecting conics.
Aligning the Haptic Bearing Surface With the Underlying Sclera Linking a series of conics (spheres and ellipses) and blending their junctions (Figure 3 a), although satisfactory for elevating the edges of GP corneal contact lenses, is far from ideal as a surface shaping tool. For example, increasing the radius of one of the segments to elevate that surface also raises all of the peripheral linked segments (Figure 3b). This technique works well enough for large scleral lenses, but for smaller scleral diameters we needed to find a better way of shaping the haptic surfaces to align them with those of the underlying sclera. We found it in spline functions.
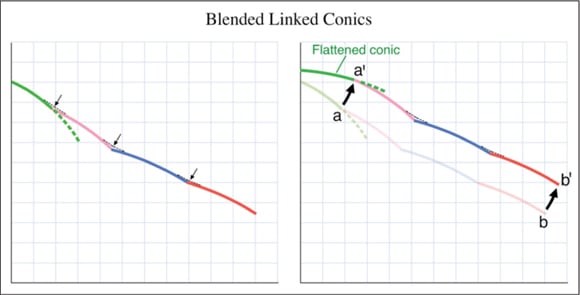
Figure 3a and b. Flattening of the radius of a conic segment also elevates the peripheral connected segments.
Splines Although formalized in the 1970s, spline functions remained a curiosity until computers capable of handling their vast numbers of recursive calculations became available. Unlike conics, which are defined by radius of curvature, the shapes of cubic splines are determined by the position (coordinates) of a series of control points through which they are required to pass through seamlessly (second order continuity). Thus their shapes are manipulated simply by moving the appropriate control points to positions that outline the desired contour (Figure 4). Making localized changes in the shape of a spline surface becomes a simple, intuitive exercise, and by definition they are always junctionless. Splines turned out to be the ideal platform for manipulating the shape of the haptic surfaces to match that of the underlying scleras.
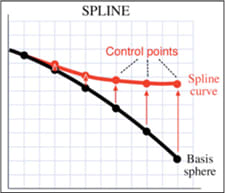
Figure 4. Scleral design with spline functions.
Controlling Corneal Clearance Avoiding all central corneal contact is an absolute requirement of the fluid-ventilated scleral lens because even slight central touch will result in compressive corneal erosions. The traditional method of controlling sagittal vault is by manipulating base curve radius or by use of reverse curves. Instead, the design of the Boston Ocular Surface Prosthesis (BOS-P, Boston Foundation for Sight) design incorporates a cubic spline in the transitional zone (between the haptic and the optic) that functions as a mathematically flexible support for the optic. Moving the proximal control points of the transitional zone vertically raises or lowers the optic, thereby enabling control of the sagittal height of the lens in precise micron increments and independently of the base curve radius (Figure 5).
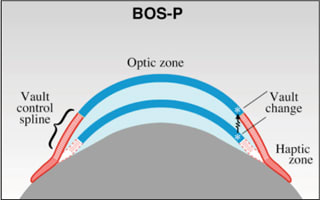
Figure 5. BOS-P design.
In addition to its ability to clear the most extreme corneal ectasia we have encountered, decoupling the base curve and the vault frees you to choose a base curve radius that offers the best balance of fitting, optics and physiology. For example, the freedom to use flatter base curves for advanced ectasia allows you to avoid high minus powers with their associated optical aberrations and increased peripheral bulk while providing larger optical zones. The result is superior quality of vision correction.
The Manufacturing Process
Other than smoothing junctions, splines are of little value in constructing scleral contact lenses if you don't have the tools for handling them in a clinically useful manner. The DTF BOS-P Designer, a powerful CAD system developed by Boston Foundation for Sight engineers over the past 15 years, is central to the unique spline technology of the Boston Ocular Surface Prosthesis. This clinically driven computer program displays and profiles the front and back surfaces of each BOS-P as spline functions that can be "bent" into virtually any desired inherently junctionless shape to, for example, eliminate zones of scleral compression. On the other hand, the haptic must also fit snuggly enough to prevent the intrusion of air bubbles that can occur when non-toric lenses are worn on toric scleras. The DTF Designer's ability to create symmetric and asymmetric toric haptic surfaces further facilitates its custom design capability.
The DTF Designer is linked to Nanoform 200 and 250 lathe/milling machines to create an integrated CAD/CAM program. These lathes, capable of generating no-polish, high-resolution, non-rotationally symmetrical surfaces, were designed to make high precision one-off parts for space stations, telescopes, etc., and their hardware and software required significant modifications to serve our specific needs. Their cost is one reason why the custom design process of the DTF technology is not commercially viable at this time.
The BOS-P Adaptive Designing Process We believe the DTF CAD/CAM technology has changed the paradigm of fitting scleral lenses. In contrast to the conventional method of selecting the best of a finite number of designs, each of which has limited modification capabilities, the DTF Designer models each device on a desktop computer and enables us to manipulate the splines of the BOS-P to accommodate the anatomical and optical features of each eye. We describe this robust customization capability as adaptive designing.Mastering the technology and clinical applications of the DTF Designer currently requires a three-month, hands-on fellowship at the Boston Foundation for Sight's facility in Needham, Mass. The BFS-certified clinician accesses the DTF CAD/CAM program in the Foundation's terminal server via the internet and custom designs each eye-specific BOS-P in real time anywhere in the world. The computer file of the lens order is automatically forwarded to the manufacturing queue where it is processed and directed to the appropriate lathe/milling machine for fabrication. Same-day manufacturing is the rule, and the devices are delivered by air express after passing stringent quality control standards.
The process of custom designing each BOS-P is time-consuming, skill-intensive, and costly, requiring a minimum of five days and the fabrication of 2.5 devices/eye on average. Professional time required for fitting eyes that have scarred bulbar conjunctivae and marginally functional corneal grafts is significantly longer and often requires the fabrication of many more devices. An overview of the BOS-P adaptive design fitting process is available at www.bostonsight.org.
Clinical Indications
Alternative to Corneal Transplant Surgery The BOS-P's superior centration, translational and torsional stability, large optical zones, and aspheric front surfaces provide a quality of vision correction often superior to that of corneal GP contact lenses. The spline-based DTF program and high resolution lathes generate optics that are virtually free of higher-order aberrations. Moreover, the BOS-P is an ideal platform for correcting residual higher-order aberrations expressed as Zernike polynomials.
The adaptive design process and customized optics have allowed us to achieve a 93 percent success rate (soon to be reported) in rehabilitating keratoconic eyes that have been intolerant of corneal GP contact lenses. ("Success" here is defined as wearing tolerance, comfort, and good functional vision for all waking hours.) Scleral lenses should virtually eliminate contact lens-intolerant keratoconus, the third commonest indication for corneal transplant surgery today — and none too soon. Keratoplasty has the least gratifying results of all major eye surgeries if measured by vision outcome. About 40 percent of penetrating corneal transplants suffer serious postoperative complications (Wagoner et al, 2009). In addition, more than a year is required after the surgery for the refractive error to stabilize and almost half of the eyes operated on for keratoconus required rigid contact lenses to provide 20/50 or better vision (Geerards et al, 2006). Moreover, fitting these warped grafts with corneal GP lenses is challenging and often impossible. In another cohort, 45 percent of grafts failed 15 years post-surgery (Williams et al, 2006) — one reason why repeat corneal transplant is the second commonest indication for this procedure. A non-invasive prosthetic device that provides immediate benefits, is free of complications, and virtually eliminates the need for surgery for these eyes has long been needed.
Managing Severe, Refractory Ocular Surface Disease Patients who have disabling and otherwise refractory ocular surface diseases are the second principal group for whom the fluid-ventilated BOS-P scleral contact lens can be life-changing. Its fluid reservoir functions as a liquid corneal bandage (LCB) for cases of devastating dry eye disease such as in chronic graft-versus-host disease, Sjögren's syndrome, Steven's-Johnson syndrome/Toxic epidermal necrolysis, corneal exposure, anesthetic (neurotrophic) corneas, and eyes exhibiting neuropathic corneal pain (pain without stain) that can result from LASIK and autoimmune diseases.
By maintaining corneal hydration and protecting fragile damaged corneal epithelium from the desiccating effects of air exposure and friction from blinking, the LCB mitigates corneal pain and photophobia. Moreover, its therapeutic oxygenated aqueous environment nurtures the healing of chronic corneal erosions and previously refractory non-infectious corneal ulcers (Rosenthal et al, 2009). Having exhausted all other treatment options, many of these patients have suffered unrelenting corneal pain and photosensitivity for years — sometimes decades. The striking relief of pain/photophobia on first applying the BOS-P, sometimes after years of suffering, is a unique emotional experience for both patient and practitioner.
Commercial Scleral Lenses
In seeking the holy grail of consistent wearing comfort, corneal GP contact lens manufacturers have begun to explore larger-diameter designs. Many have been too conservative in departing from tradition and have begun to test the feasibility of corneo-scleral and small scleral lenses. However, they may find, as we did, that halfway measures are often disappointing.
Large-diameter corneal lenses do not create an LCB and tend to become adherent as their underlying stagnant tear layer fills with glue-like mucin secreted by the epithelium that retracts, pulling the lens against the cornea with increasing force. Corneo-scleral lenses are also vulnerable to adhesion, which can traumatize the cornea even more than corneal lenses can — I have observed the more prominent junction between their optic and haptic become wedged into the cornea, thereby eroding the corneal surface and, in some cases, triggering peripheral corneal neovascularization.
With smaller scleral lenses (that by definition rest entirely on the sclera), the major obstacle becomes the small bearing scleral footprint. Small scleral lenses may create excessive scleral compression and are prone to developing suction. We believe large scleral lenses represent a far better opportunity for the commercial laboratories.
The Need Is Evident
The personal, societal, and economic costs of corneal disease are enormous. There are hundreds of thousands of patients in the United States alone who could benefit from modern scleral lenses. Many have no other options for regaining functional vision or for finding relief from constant, disabling eye pain. For others, scleral lenses avoid the need for keratoplasty. Yet eyecare professionals and commercial GP lens manufacturers have been slow to embrace a device that is changing the landscape of managing some of the most devastating corneal diseases.
The Boston Foundation for Sight, a 501(c)3 nonprofit organization, provides free care to approximately 20 percent of its patients and substantially subsidizes the fitting costs of the remaining 80 percent. Nevertheless, we and our affiliated clinics turn no one away because of inability to pay. This is not a for-profit business model. Yet commercial laboratories have a critical role to play if we are to meet the needs of patients for whom modern GP scleral lenses are their only hope for rejoining mainstream society.
We believe that lenses in which the haptic bearing surface is designed with serial conics generally work best when fabricated in larger diameters (20mm or greater). Because the effects of scleral toricity increase with its distance from the limbus, large scleral lenses require toric haptics more often and in greater amounts compared to smaller scleral lenses. Fortunately, this technology is not rocket science.
However, the weakest link in the commercial model is the lack of skilled scleral lens fitters. The fitting principles of scleral lenses are different from those for corneal GP contact lenses. In fact, we've found that learning to fit these devices is facilitated by a mindset unencumbered by prior contact lens experience. Because the process of designing each device in the commercial sector is done by narrative communications between the fitter and laboratory personnel, the technical language used for this is critical and industry-wide standards are essential.
Above all, state-of-the-art generic teaching resources must be developed to train scleral lens fitters. This is feasible because there are basic fitting principles common to all scleral lenses. Scleral lens fitting should become a recognized and fairly compensated subspecialty.
We believe the best vehicle for achieving these goals is through a non-profit umbrella organization supported by a membership of scleral lens manufacturers with appropriate representation from the eye-care professions. The Boston Foundation for Sight would be honored to be a founding member. Currently our international partners include two clinics in India; L.V. Prasad in Hyderabad and a nonprofit clinic in Mumbai, and one in Nagoya, Japan. Partners in the United States include the Brooke Army Medical Center, San Antonio, Texas; Cullen Eye Institute, Baylor Medical College, Houston, Texas; Doheny Eye Institute, University of Southern California, Los Angeles; and Massachusetts Eye and Ear Infirmary, Harvard, Boston, Mass. We are continuing to expand our network of nonprofit affiliated clinics in academic tertiary eyecare centers in the United States and internationally. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #169.