


THERAPEUTIC UPDATE
New Anti-Infective and Anti-Inflammatory Medications and Trends
Four recent medications are helping to bring faster relief to our patients.
By Paul Karpecki, OD, FAAO

Dr. Karpecki is clinical director of Corneal Services and Ocular Surface Research at the Koffler Vision Group-Kentucky Center for Sight. He is a paid consultant to Allergan, B&L, TearLab, AMO, OcuSoft, Odyssey Medical, Focus Labs, Inspire Pharmaceuticals, and Sirion Therapeutics but has no financial interest in any of the products mentioned in this article. |
New anti-infective and anti-inflammatory medications continue to enter the market, often providing such benefits as greater effectiveness and a longer period of effectivity. This article will focus mainly on four such medications, their indications, mechanisms of action, and dosing schedules.
1. AzaSite
AzaSite (azithromycin 1.0% in a Dur-aSite [InSite Vision] vehicle) from Inspire Pharmaceuticals was approved for treating bacterial conjunctivitis. The DuraSite vehicle allows the azithromycin to remain in solution and also increases the drug contact time. But it is the azithromycin molecule that makes this drug effective because of its inherent properties.
Azithromycin has broad-spectrum activity, but the unique characteristics are its ability to accumulate in ocular tissue such as the conjunctiva and eyelids. Although approved for bacterial conjunctivitis, many practitioners have used it off-label for blepharitis, likely because the penetration and accumulation of drug in the eyelid tissue is very significant. In research involving rabbits, AzaSite demonstrated a 125-hour half-life and was still present in high doses 12 days into the study, although the drug was used only for seven days and only once a day for five of those days (Akpek et al, 2009).
It is a combination of AzaSite's ability to penetrate tissue and the long residence time that appears to be why practitioners are finding success with its use in lid margin disease management, but some research also points to significant anti-inflammatory properties similar to that of tetracycline medications. Blepharitis, with a related inflammatory component, is thought to be associated with contact lens intolerance, so this pharmaceutical might also prove useful in treating lens wearers who experience discomfort symptoms.
Dosing for bacterial conjunctivitis follows the clinical trial data at b.i.d. for two days followed by q.d. for an additional five days. For off-label use in blepharitis, most practitioners are recommending b.i.d. for one-to-two days and then q.d. for an additional two-to-four weeks depending on the severity of the lid margin disease. Pulsed dosing periodically throughout the year is incorporated in chronic cases of blepharitis.
2. Durezol
Durezol (difluprednate ophthalmic emulsion) 0.05% from Sirion Therapeutics is an ophthalmic emulsion that was originally a dermatological preparation and is the newest strong steroid to receive U.S. Food and Drug Administration (FDA) approval. It was approved for treating inflammation and pain associated with ocular surgery and is the first steroid to receive a specific indication that includes pain along with inflammation. The potency of this corticosteroid can be attributed to its molecular structure including the fluorination at C6 and C9 attached to a prednisolone derivative. The emulsion is an oil-in-water mixture, which has allowed traditionally poorly soluble drugs, such as prednisolone, to dissolve in the oil phase (castor oil). It also eliminates the need for shaking the bottle and allows a more consistent amount of drug in each drop compared to a suspension.
Off-label use for iritis and uveitis management has demonstrated significant clinical success at an even lower dosing (DaVanzo, 2009). In one study comparing Durezol q.i.d. to Pred Forte (prednisolone acetate solution, Allergan) q2h, Durezol was equivalent to Pred Forte at clearing anterior chamber cells, even when dosed half as often. In addition, Durezol was numerically superior at several other efficacy parameters, including measurements related to anterior chamber cell and flare and symptoms including pain and photophobia (Jamal and Callanan, 2009).
In previous uveitis clinical trials, Durezol was equally effective to betamethasone and was significantly better at clearing the inflammation in patients who have more significant uveitis including panuveitis. Betamethasone is not available in the United States, but research has shown that it is six times more potent than prednisolone drops (Jamal and Callanan, 2009). As with any strong steroid, there are known risks of intraocular pressure (IOP) elevation. Durezol has no benzalkonium chloride (BAK) in the formulation.
3. Besivance
In July 2009, the FDA approved Besivance (besi-floxacin 0.6%) from Bausch & Lomb for the treatment of bacterial conjunctivitis. Besivance has demonstrated success in eliminating ocular pathogens, including methicillin-resistant Staphylococcus aureus (MRSA), in microbiological studies (Sanders et al, 2009).
This drug is the first chlorinated fluoroquinolone to come to market and is also the first ophthalmic fluoroquinolone that has no systemic counterpart. The significance of this is the potential for less resistance. It is believed that much of the resistance in medicine today, including resistance to older fluoroquinolones, results from the use of the oral medications in hospital settings and in agriculture. Without a systemic besifloxacin medication, resistance to the ophthalmic medication may be less likely.
Besivance also uses the DuraSite vehicle to allow a longer drug release time. With a concentration of 0.6%, this allows for significant drug to be present on the ocular surface over an extended period of time. The labeled dosing is three times a day every four-to-12 hours. You may prescribe the medication every 12 hours for bacterial conjunctivitis, or in offlabel use for surgical prophylaxis at six-to-12-hour intervals or at higher dosing levels for a keratitis.
In terms of the molecular structure, the C8 chlorine component of the besifloxacin molecule provides enhanced and equal inhibition of DNA gyrase and Topoisomerase IV. By equal inhibition, there is less chance of resistance via one of the two enzyme pathways. Additionally, its C7 aminoazepinyl component is thought to contribute to broad-spectrum activity against grampositive organisms in particular. Research has also pointed to potential anti-inflammatory properties, which may be why it is so well tolerated by patients and why it is quick to eradicate bacterial pathogens (Zhang et al, 2008).
One in vitro study of 2,690 clinical isolates from 40 species of bacteria showed that the minimum inhibitory concentrations for besifloxacin were at least two-to-four times lower than that of the other antibiotics tested including previous fluoroquinolones (Haas, 2009). Most notably, besifloxacin proved effective against gram-negative and gram-positive pathogens including MRSA, which is of significant concern in medicine today.
4. Zirgan
The most recent FDA approval also came in July for Zirgan (ganciclovir ophthalmic gel) 0.15% from Siri-on Therapeutics for treating Herpes Simplex Virus (HSV) keratitis (Figure 1). This is the first anti-viral medication to be FDA-approved in decades and is a welcome addition to the armamentarium of anti-infective medications. The FDA granted orphan drug designation to Zirgan in 2007, which allowed a relatively rapid FDA approval process for the treatment of acute herpetic keratitis or dendritic epitheliopa-thy. HSV keratitis is one of the leading causes of corneal transplants, and there are approximately 50,000 new and recurrent cases of HSV keratitis each year.
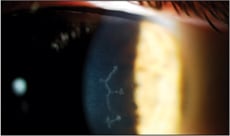
Figure 1. Herpes Simplex Virus dendritic ulcer.
The drug, which has long been available in Europe under the name Virgan, has been the standard of care treatment for HSV keratitis for more than a decade. It works by selectively targeting the replication of HSV DNA within corneal cells. The advantage of Zirgan is that it targets only the infected cells as opposed to previous antiviral medications that affected both healthy and infected cells. In the clinical trial, clinical resolution of HSV corneal ulcers occurred in 77 percent of subjects by day seven (compared to 72 percent for topical acyclovir, the drug in the other arm of the study) (Hoh et al, 1996). The recommended dosage is five times per day until the dendritic ulcer heals and then t.i.d. for seven days. The lower dosing regimen will also be an advantage over other antiviral medications. Zirgan will likely become available to U.S. practitioners in early 2010.
Case Grand Rounds
Case #1: Bacterial Keratitis A 26-year-old Caucasian male presented with a foreign body sensation, light sensitivity, and a red eye that began that morning. He was a long-term contact lens wearer. Slit lamp examination revealed a 2+/3-conjunctival injection, slight edema, normal pupils, and a small peripheral infiltrate with staining over the infiltrate. The anterior chamber revealed Grade 2 cells and flare (Figure 2). It appeared to be a sterile infiltrate, but an anterior chamber reaction was present.
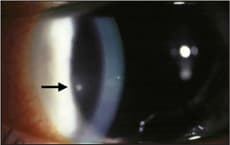
Figure 2. Corneal infiltrate from bacterial keratitis in Case Grand Rounds case #1.
Patients who have bacterial keratitis experience symptoms of acute onset, pain, photophobia, mucopurulent discharge, and decreased vision. Clinical signs may include conjunctival hyperemia and ciliary flush, lid edema, tear film debris (thick tear film with cells), an epithelial defect, a grayish-white stromal infiltrate, and an anterior chamber reaction (from few cells to a hypopyon). Table 1 provides the differential diagnosis between a sterile infiltrate and an infectious corneal ulcer (Figure 3).
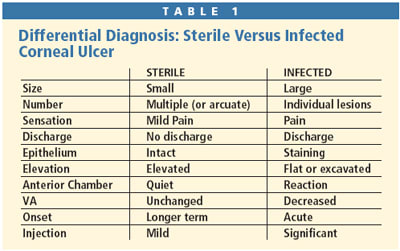
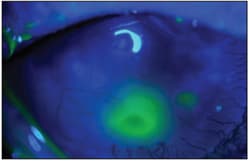
Figure 3. An infectious corneal ulcer with overlying staining.
In this case a broad-spectrum antibiotic such as a fluoroquinolone should be prescribed. Popular fluoroquinolones prescribed in these cases have included Zymar (Allergan), Iquix (Vistakon Pharmaceuticals), Vigamox (Alcon), and now Besivance. Typically a loading dose is provided every 15 minutes for two hours (or every five minutes for 30 minutes) followed by dosing every hour while awake and then either every two hours during the night or prescribe bacitracin or tobramycin h.s.
Case #2: Epidemic Keratoconjunctivitis (EKC) The management of EKC has gone through changes because it can be a very painful and photophobic condition and few therapies have been effective. Practitioners have tried Viroptic (Monarch Pharmaceuticals) but there is nothing in the literature or in clinical experience to suggest that it works for EKC. Corticosteroids help with the pain and discomfort, but it is also possible that such medications lengthen the disease course. So what is the treatment for this relatively common but difficult to treat condition?
Some doctors have used Betadine (Purdue Pharma) as an off-label application to treat EKC patients. According to anecdotal reports by well-respected clinicians, the Betadine treatment approach greatly helps EKC patients and may even prevent the potential of sub-epithelial infiltrates later in the course of the disease. The regimen is as follows:
- After ensuring that the patient doesn't have an allergy to iodine, instill proparacaine to anesthetize the cornea because Betadine stings on application.
- Instill four drops of Betadine 5% solution on the eye; have patients close their eyes and roll them around to ensure uniform distribution of the drops on the ocular surface (one-to-two drops of a nonsteroidal anti-inflammatory drug [NSAID] can be instilled prior to Betadine).
- One minute later, rinse the eye with sterile saline solution or irrigating solution.
- Instill one or two drops of an NSAID (such as Xibrom [Ista Pharmaceuticals], Nevanac [Alcon], or Acuvail [Allergan]) and have patients continue with the NSAIDs q.i.d. for one week. With the virus now eradicated because of the Betadine, the remaining conjunctival inflammation must be managed. A corticosteroid such as loteprednol 0.5% q.i.d. for one week is effective.
In the future, another option will exist; as mentioned previously, in early 2010 we are likely to see the arrival of Zirgan. In Europe this is the drop of choice for HSV and it may also provide a good therapeutic option for EKC and other viral conditions including dermatological lesions around the eyes. It will be interesting to see how effective it will be once we can gain experience with it in the United States. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #169.