


POST-SURGICAL CORNEAS
Fitting Challenge: Post-Surgical Corneas
You can manage these tough fits with tools already in your practice.
By Randy Kojima & Fern Yee, OD

Randy Kojima is the Director of Technical Affairs for Precision Technology in Vancouver, Canada and a research scientist and clinical instructor at Pacific University College of Optometry in Forest Grove, Ore. You can reach him at randy@ptsoptics.com. 
Dr. Yee is a graduate of Pacific University College of Optometry. She has an independent optometric practice in Austin, Texas. |
One of the more challenging contact lens fits that we face is the post-refractive surgery cornea. When the visual outcome is not as desired, patients look to us for help.
Often we're able to correct refractive shortcomings with soft spherical or toric lenses. However, what if the patient has high degrees of asymmetrical astigmatism, aberrations and poor visual acuity? The answer is simple — GP lenses, right? But you now have a cornea that is flatter centrally, steeper in the midperiphery and then flatter again near the limbus. In other words, your cornea is the reverse of its normal geometry. What should your approach be to provide both fit and vision on this very challenging corneal shape?
Understanding the Shape
The shape of a normal cornea can be described as a prolate ellipse. This means that the steepest radii of curvature is central or apical. As you travel from the apex to the limbus, the corneal curvature progressively flattens. This prolate or progressively flattening cornea is characteristic of most normal, nonsurgical, trauma-free corneas (Figure 1).
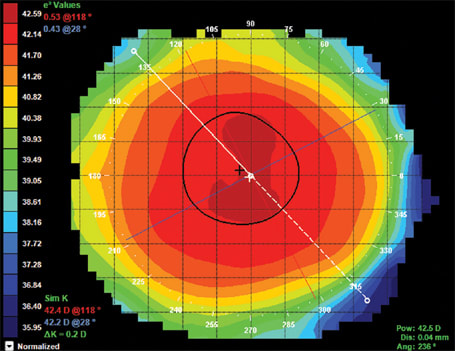
Figure 1. Normal prolate spherical cornea with the steepest radii of curvature at the apex (warm colors) with progressively flatter shape out to the periphery (cooler colors).
Conversely, post-refractive surgery eyes that underwent myopic reduction are often rendered oblate in shape. The higher the desired myopic reduction, the more oblate the cornea becomes. The resulting cornea is now flat at the apex (treatment zone) and steeper paracentral to the apex before flattening again near the limbus beyond the surgically altered zone (Figure 2).
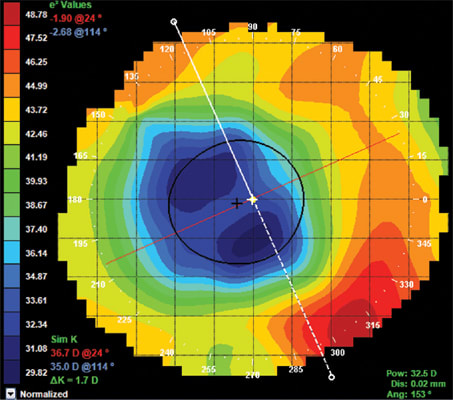
Figure 2. Highly oblate post-RK patient with flatter central curvature compared with steeper midperipheral shape (OD).
It is possible for a post-surgical outcome to result in less than ideal visual acuity. If enhancement of the procedure is not an option, then glasses or contacts lenses are required to correct the residual prescription. In many cases, spherical or toric soft contact lenses can provide quality vision. However, when the resulting cornea has irregular astigmatism or increased higher-order aberrations, often only a GP contact lens will provide an acceptable or ideal level of visual acuity.
If a GP lens is the best option, then the challenge becomes fitting an oblate cornea. Is it more important when fitting such a cornea to achieve alignment in the center where the cornea is flat or to achieve alignment in the periphery where the cornea is steep? As you can imagine and as we've already stated, the shape of a post-surgical oblate eye is reverse of a normal prolate cornea.
A Case Study
A 50-year-old male who had radial keratotomy (RK) surgery 17 years ago presented to the office. Approximately five years ago, the patient noticed his vision was starting to change and was reluctant to undergo additional surgical procedures. He presented to the office wearing glasses and was looking to improve his quality of vision with either glasses or contact lenses.
His manifest refraction was OD +8.00 –3.50 × 135 (20/25) and keratometry readings were 43.50/46.70 @ 24. Although this patient had bilateral RK, here we'll focus on the fitting of the right eye as it represented the higher of the two prescriptions.
The patient's corneal topography revealed the expected oblate post-surgical shape of the cornea (Figure 2). Note that the treatment zone (blue area of central flattening) is displaced temporal to the visual axis of the eye. Additionally, the asymmetry of the treatment zone and irregular shape of the astigmatism could be contributing to the instability and reduced quality of vision.
He had tried soft contact lenses in the past, but they did not provide good vision. Given the asymmetrical nature of the treatment zone, a GP lens would be required to produce a more ideal anterior surface. By employing a topographer's contact lens fitting software (Medmont E300 corneal topographer, Precision Technology Services, Ltd.), we were able to design and predict the fit of a spherical GP lens for this challenging cornea. Figure 3 shows a GP sphere fit 0.25D steeper than K on our 2.25D corneal cylinder. The fitting software shows that we can achieve an acceptable apical clearance (29 microns). However, the problem would be the excessive edge lift over the steeper paracentral cornea (>200 microns). A lens with such a fitting relationship would likely exhibit poor centration, stability, comfort and vision.
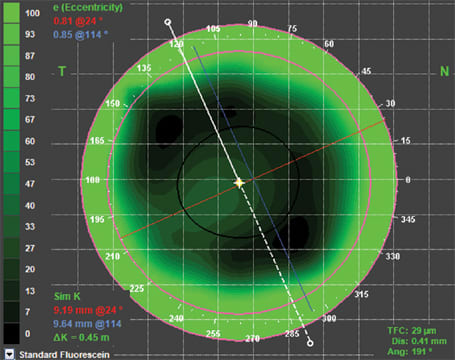
Figure 3. Spherical GP OD on our patient. Medmont software predicts an acceptable apical clearance (29 microns) with a base curve 0.25D steeper than K. However, an excessively wide and deep edge lift (>200 microns) surrounds the area of central alignment.
To eliminate the problems created by aligning centrally on the oblate shape, what about fitting for peripheral alignment? By selecting a base curve significantly steeper than K, we can achieve peripheral alignment at 10 o'clock and 4 o'clock on this asymmetrical oblate shape (Figure 4). However, we can observe that by aligning in the periphery, our spherical lens produces excessive apical clearance and a likely air bubble over the "depressed" central cornea (103 microns of central tear film thickness).
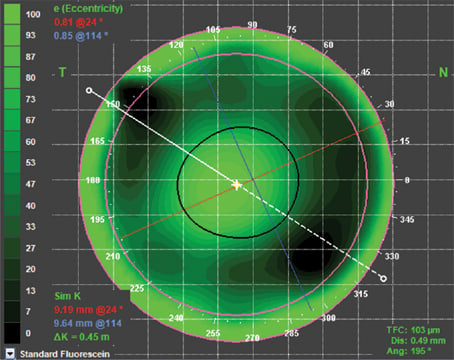
Figure 4. A spherical lens designed to align in the periphery on our oblate post-surgical cornea; however, excessive apical clearance (103 microns) would result by aligning peripherally.
As stated previously, the shape of an oblate cornea is flat centrally, steeper in the midperiphery and then flatter nearer to the limbus. The oblate cornea is reverse in geometry to normal, nonsurgical eyes and requires a reverse geometry shape for the back surface of the lens. Most GP laboratories provide reverse geometry fitting sets for such corneas because it's nearly impossible to accurately fit these patients empirically. By diagnostically fitting a reverse geometry lens similar in shape to the reverse geometry cornea, we can often achieve a successful fitting relationship with one custom order attempt.
The question is where do we start in parameter selection? You may already have the ideal tools to help answer this question. A corneal topographer is a critical instrument to aid you in best selecting the initial lens. Secondly, if you practice orthokeratology, you may already have the ideally shaped lens in your fitting set to use as a diagnostic contact lens.
A method that is fundamentally similar no matter what tools you have is to look at the cornea mathematically. First, you must match the sagittal height of the lens to the sagittal height of the cornea. In other words, does the lens approximate the shape of the cornea, providing an adequate apical clearance? Second, you must determine what peripheral alignment (curve or angle) will produce good centration, comfort and physiological response.
A number of topographers will allow you to measure the sagittal height of the cornea. Although it's rare for us to think of contact lenses in this way, matching the sagittal height of the lens to the sagittal height of the cornea ultimately produces all ideal contact lens fits. The Medmont E300 topographer will allow you to measure the sagittal height of a cornea over a designated chord diameter. On our patient, we measured the height of the cornea at 1,543 microns (1.543mm) over a chord diameter of 9.35mm. Allowing for a small amount of tear layer at the apex between the lens and cornea (20 microns), the ideal lens sag would be 1,543 microns + 20 microns = 1,563 microns.
From this value, we can check the manufacturer's table for the sagittal height of each orthokeratology (reverse geometry) lens. In this case, we had access to the BE Retainer design (Precision Technology Services, Ltd.), so we used the fitting software to select the closest diagnostic lens to our target sagittal depth, which was the 8.25mm BE Retainer Diagnostic (1,565 microns or 1.565mm).
The first consideration in fitting reverse geometry lenses on oblate eyes is to determine which lens parameters will achieve peripheral alignment, centration and comfort. You can steepen or flatten the base curve of the lens to achieve the ideal apical clearance. However, it's critical to know the peripheral parameters that will produce an optimum fitting outcome from the perspective of centration and comfort. In other words, reverse geometry lenses are fit from the outside in rather than the opposite, which is how we fit normal geometry lenses.
Upon dispensing, the 8.25mm diagnostic lens exhibited excessive movement and was uncomfortable. Considering that peripheral alignment, centration and comfort is desirable, the initial outcome indicated that the diagnostic lens was too flat, so we selected the next steeper lens from the fitting set. The steeper 8.20mm diagnostic lens aligned well in the periphery, centered and was comfortable to the patient (Figure 5). Because we have now determined the correct "outside" parameters, we can now evaluate the "inside" parameters.
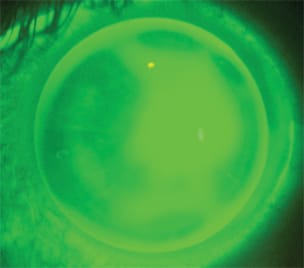
Figure 5. 8.20mm BE Retainer diagnostic lens exhibiting good peripheral alignment and apical clearance on an oblate post-RK cornea.
The fluorescein pattern exhibited a fair amount of apical clearance over the flattened central cornea, although it was not excessive because bubbles weren't present. An over-refraction on the plano diagnostic lens revealed –1.25D, which provided the patient with 20/25 vision.
To be certain that we tried all potential parameter combinations while the patient was in the chair, we attempted the next steeper diagnostic lens (8.15mm). This lens exhibited good peripheral alignment and centration similar to the 8.20mm lens. The patient also reported that the perceived comfort was the same. However, the steeper diagnostic lens increased the apical clearance, which decreased the visual acuity to 20/50 with an over-refraction of –1.00D. We determined that either the 8.15mm or 8.20mm lenses had the correct peripheral alignment parameters and that the 8.15mm base curve would need to be flattened to reduce the central clearance and improve visual acuity. Because the second diagnostic lens had performed well in all the categories, we ordered the parameters of an 8.20mm BE Retainer lens with a power of –1.25D.
Upon dispensing, the patient's custom lens centered well with a slight temporal displacement (Figure 6), which followed the lateral asymmetry of the baseline cornea. The lens shared its bearing over a broad circumference of the peripheral cornea, which resulted in an acceptable fit and comfort. Although the visual acuity could not be improved beyond 20/25, the patient reported that the quality and stability of vision was noticeably improved compared with glasses and previous soft lens wear.
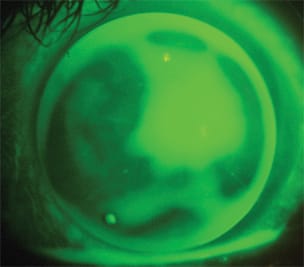
Figure 6. Custom ordered BE Retainer lens designed for orthokeratology but adapted for the post-surgical oblate cornea.
Fitting Pearls
Oblate, post-surgical corneas are clearly among the most challenging of contact lens fits. This shape of eye requires an incredibly precise fitting that, when achieved, can result in good comfort, physiological response and visual acuity. A corneal topographer can be instrumental in determining a starting point for lens design parameters that won't result in a lengthy diagnostic trial.
Many practices already have orthokeratology diagnostic lenses that are ideal for many of the post-refractive surgery oblate eyes. As an advanced fitting concept, practitioners can measure the sagittal depth of the cornea with the corneal topographer and compare this value to known orthokeratology diagnostic lens depths. This method will save you much time and effort during the trial process.
Finally, fit oblate eyes from the outside in. Determine the lens that will fit well in the periphery to achieve good centration, alignment and comfort. Then evaluate the apex and simply steepen or flatten the base curve to increase or decrease the apical clearance while maintaining the same peripheral parameters (reverse curves and alignment zone). CLS