


SCLERAL LENS DESIGN
Fitting Techniques for a Scleral Lens Design
This scleral lens design can help mask extreme corneal irregularity and provide therapeutic benefits.
By Gregory W. DeNaeyer, OD, and Robert Breece, OD

Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio. His primary interests include specialty contact lenses. He is also a consultant or advisor to MedLens Innovations, Inc. and Essilor. He may be reached at gdenaeyer@arenaeyesurgeons.com. 
Dr. Breece is the president and lens design consultant for MedLens Innovations, Incorporated in Front Royal, Virginia where he has a specialty contact lens practice. He is the inventor of the Jupiter scleral lens as well as other rigid and soft contact lenses for difficult cases. He is also a consultant or advisor to Essilor. |
Modern scleral contact lens fitting has evolved significantly since scleral lenses were introduced in the late 19th century. Diagnostic lens fitting and GP materials have revolutionized this lens modality. By definition, scleral contact lenses are greater than 18mm in diameter, which differentiates them from miniscleral, semi-scleral, corneal-scleral and corneal GP lenses.
Scleral contact lenses are fit to align and rest upon the scleral conjunctiva, completely vaulting the corneal surface. The difference in sagittal depth between the contact lens and the eye determines this relationship (Figure 1). This is in contrast to corneal GP lenses for which you determine the fit by the base curve-to-keratometry measurement because they are fit to align with the cornea.
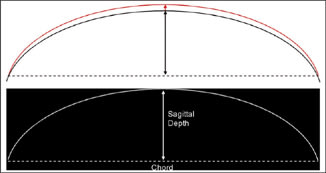
Figure 1. Relative sagittal depth differences between contact lens and eye (top). Sagittal depth (bottom).
Jupiter Scleral Contact Lenses
The Jupiter scleral contact lens (Medlens Innovations, Inc./Essilor) is designed as a semisealed lens that does not need to closely align with the cornea. Its advantage over smaller contact lens designs is that it can trap a large volume liquid reservoir that not only can mask extreme corneal irregularity (Figure 2), but can also be therapeutic for patients who have corneal/scleral disease.
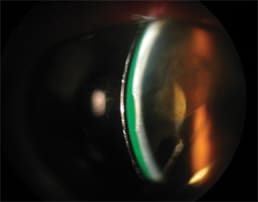
Figure 2. Cross section of a Jupiter lens masking extreme corneal irregularity secondary to a corneal scar.
Jupiter lenses are manufactured in either Tyro 97 (Lagado Corporation) or Boston XO (Bausch & Lomb) and should be plasma-treated as this enhances wetting. Tear exchange occurs through peripheral lens flexure secondary to blinking. Fenestrations are rarely used for true scleral lenses because they do not aid in tear exchange and will often result in bubbles underneath the lens.
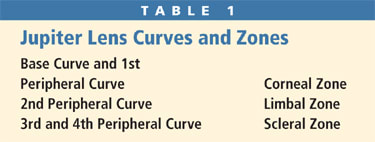
The Jupiter scleral lens has five curves organized into three zones (Table 1). Toric scleral zones are available to enhance the alignment on eyes with very irregular scleras. However, these contact lenses can have a fair amount of flexibility in the scleral zone, so toric peripheries are rarely needed. Jupiter lenses use aspheric optics to help reduce spherical aberrations and enhance visual acuity.
Indications
Consider scleral lens fitting with the Jupiter lens to fit extremely irregular corneas that have conditions such as advanced keratoconus, trauma or post-surgical irregularities secondary to a graft, RK, PRK and LASIK. Scleral lenses are ideal for patients for whom a smaller GP lens will not center or when an unhealthy compromise exists between bearing and vault of the cornea (Figure 3).
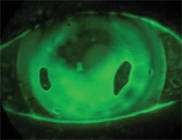
Figure 3a. Mini-scleral lens (15.0mm) on a corneal transplant with compromise between bearing and excessive clearance.
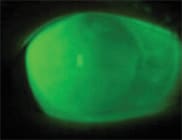
Figure 3b. Scleral lens (18.8mm) on the same eye vaulting the corneal transplant without touch or bubbles.
Also consider Jupiter lenses for patients who have compromised corneas and/or scleras secondary to severe dry eye syndrome, Stevens Johnson syndrome, graft versus host disease and neurotrophic keratitis, especially if soft lenses have failed.
Fitting the Jupiter Scleral Contact Lens
To successfully fit the Jupiter scleral contact lens, you must meet three objectives. The lens must vault the central cornea, achieve complete limbal clearance and align with the scleral conjunctiva. The amount of clearance is based on relative sagittal depth, which you can best determine by using diagnostic lenses. The basic trial set has 14 lenses with differing base curves (labeled in diopters) and a standard peripheral curve design. Advanced sets are also available that incorporate reverse geometry designs and advanced keratoconus designs.
The first step of the fitting process is to choose an initial diagnostic lens. Using topographical data, select a base curve equal to the steepest corneal curvature plus one diopter. If reliable corneal topography data is not available, select the 48D lens to start with, as this will vault most corneas. Keep in mind that relative sagittal depth, and not just the steepness of the base curve, determines the amount of clearance (the steepness of the base curve in-part determines the sagittal depth). This is why a scleral lens with a 48D base curve could in some cases easily vault a cornea that has a 52D steep topographical area. The reason is that even though the cornea has a steeper dioptric value, the overall sagittal depth of the cornea and sclera may be relatively flatter than the overall sagittal depth of the 48D lens.
With the initial diagnostic lens held concave side up, instill saline solution into the lens and add a small amount of fluorescein. Have patients tilt their head down and centrally apply the lens so that the solution remains in the lens. A yellow wratten filter with cobalt illumination is essential to accurately evaluate fluorescein patterns because the filter greatly enhances the fluorescein. Another way to determine the amount of clearance is to use a slit beam to view the contact lens, reservoir and cornea in cross-section (as in Figure 2).
You can now evaluate the three zones of the lens. First evaluate the corneal zone, which includes the base curve and first peripheral curve. A scleral lens that is too flat will rest upon the cornea and show little or no fluorescein in this area. To correct this, choose a steeper base curve. A lens that is too steep will show excessive fluorescein under the central area. Select progressively flatter lenses until any area in the corneal zone almost touches the cornea. This is called the vault reduction method (Figure 4). With this last lens in place, let the lens settle for approximately 20 minutes. Some scleral lenses will settle into the conjunctiva, which will decrease the overall sagittal depth and result in potential central touch. Reverse geometry lenses may be required to vault midperipheral touch, as is often the case with oblate corneas.
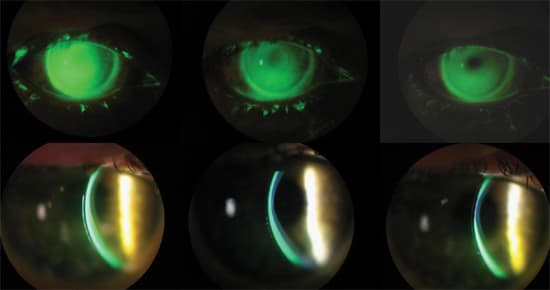
Figure 4. Vault reduction method – a 48D, 46D, and 44D lens on a keratoconic cornea.
Next evaluate the limbal zone. Complete and generous limbal clearance is necessary to ensure tear circulation and prevent erosive damage to the limbal epithelial cells (Figure 5a). If you observe very little fluorescein in the limbal area of the lens (Figure 5b), then the lens is too small and you should select a larger diameter.
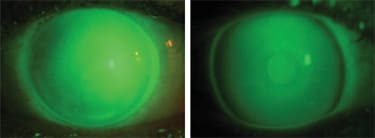
Figure 5a (left). Scleral lens with complete limbal clearance. 5b. Scleral lens with inadequate limbal clearance.
Finally, evaluate the scleral zone and lens edge. The lens should rest evenly on the scleral conjunctiva with the edge appearing just above the conjunctival epithelium (Figure 6). The lens should not move with blinking. A lens that moves will actually be uncomfortable to the patient. You can correct this by tightening the scleral zone. No fluorescein will be visible under a well-fit scleral zone except at the edge. If you observe blanching (Figure 7) or severe conjunctival compression, order a flatter scleral zone.
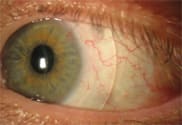
Figure 6. Scleral zone.
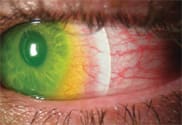
Figure 7. Blanching secondary to tight scleral zone.
With the-best fit diagnostic lens on the patient's eye, determine the lens power by a sphero-cylindrical over-refraction. A cylinder component in the over-refraction or non-spherical keratometry readings of the lens on the eye usually indicates lens flexure, which you can correct in the final design by increasing the center thickness.
Application and Removal
Successful application of the Jupiter scleral lens requires that it be rinsed and filled with saline prior to placement on the patient's eye. Use only non-preserved saline solution. Tear circulation with scleral contact lenses is reduced, so there is an increased risk of toxicity because preservatives are in contact with the cornea for a longer period of time.
Instruct patients to lean forward and tilt their head down to place the scleral lens on the eye so that the solution remains in the lens. Patients can handle the lens with either a DMV classic plunger or by balancing the lens in a tripod between the thumb, index and middle fingers. Small insertion bubbles are of no consequence, but larger bubbles will disrupt both vision and comfort.
Removal of the scleral lens is usually performed using a plunger. Because the Jupiter lens is large, the capillary forces that hold the lens on the eye are powerful, so removal is always best accomplished by placing the plunger on the inside edge of the lens, which eliminates suction as the lens is pulled away. The Jupiter lens may also be removed by using the lower lid to lift the contact lens edge.
Case Examples
Patient #1 was a 39-year-old male who reported for specialty contact lens evaluation. He had a history of keratoconus and had been unable to wear his left GP contact lens because it was uncomfortable and would not stay in his eye. Topography showed severe irregularity, and slit lamp evaluation revealed 3+ Vogt's striae.
We fit the patient with a Jupiter scleral contact lens with a diameter of 18.2mm, base curve of 52D, and a power of –9.25D (Figure 8). He is able to see 20/25 with the lens in place and enjoys all day comfort.
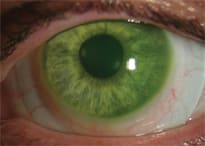
Figure 8. The Jupiter scleral lens on Patient #1.
Patient #2, a 46-year-old white female, reported for evaluation of decreased vision OS. She had a history of bilateral RK surgery 18 years prior. Best acuity in her left eye with a hyperopic astigmatism correction was 20/80. Slit lamp exam showed eight thickened radial RK cuts and one astigmatic cut of the left eye. An area of ectasia was evident inferior temporal. Topography was unable to be computed, but a mire pattern confirmed this ectasia and irregularity.
After failing in a hybrid contact lens design, we fit the patient with a Jupiter scleral lens with an 18.2mm diameter, base curve of 51D, and a power of –15.75D (Figure 9). Her acuity with the contact lens in place is 20/25 and she is able to wear the lens comfortably all day.
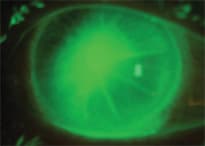
Figure 9. Fluorescein pattern of scleral lens on Patient #2.
Conclusion
The most difficult issue with respect to fitting conventional corneal GP lenses on irregular corneas is achieving proper lens centration. A lens that decenters not only degrades potential acuity, but is uncomfortable to wear. Jupiter scleral lenses are advantageous in that they eliminate these issues. Because the lens is able to hold a large liquid reservoir, it can mask extremely irregular surfaces while acting as a therapy for a compromised cornea. We've found from our experience that the Jupiter scleral lens is comfortable to wear, and vision is stable because it rests on the scleral portion of the eye without movement. Modern fitting processes allow clinicians with training and a fitting set to use these lenses in their practices. CLS