


dry eye dx and tx
The Limbus: A Stem Cell Microenvironment
BY KATHERINE M. MASTROTA, MS, OD, FAAO
As eyecare practitioners, we sometimes take for granted the incredible healing ability of the cornea. With confidence, we expect that corneal abrasions will heal quickly, the wound replaced with a new, smooth, and optically clear system of cells. Even under normal conditions, the corneal epithelial surface is a self-renewing biological continuum. Continuous renewal of the corneal epithelium is vital for preserving a smooth, transparent, refractile surface necessary for clear vision and ocular comfort. Let's consider how this happens.
The Renewing Process
Pluripotent, undifferentiated stem cells are present in all selfrenewing body tissues and maintain a steady-state population of healthy cells. The stem cells of the corneal epithelium are situated at the limbus, nestled within the undulating folds of the Palisades of Vogt (Figure 1).
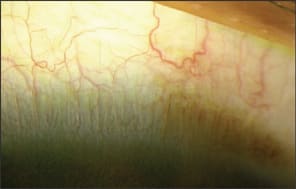
Figure 1. A small portion of the limbus: note the ridges and pigment characteristic of the Palisades of Vogt.
The limbus is a narrow annular transition zone that separates the anatomically contiguous, yet phenotypically different cells of the conjunctival and corneal epithelium. It has a distinct histological architecture. It differs from conjunctiva in that it is devoid of goblet cells, and unlike the optically clear corneal epithelium, it has Langerhan's cells, melanocytes, and underlying blood vessels.
Maintaining homeostasis and corneal epithelial cell turnover, stem cells in the limbus divide to produce a daughter stem cell and a transient amplifying cell (TAC). TACs migrate centrally within the cornea to occupy its basal layer. Subsequent cellular divisions give rise to postmitotic cells, which reside in the suprabasal layers. Progressive differentiation of postmitotic cells results in terminally differentiated cells (TDCs) in the superficial corneal epithelial layers. TDCs are non-keratinized, stratified squamous corneal epithelial cells. These cells are continually sloughed away from the corneal surface and replaced by maturing, underlying cell layers.
Limbal stem cell function is modulated by developmental, hormonal, neuronal, vascular, and inflammatory factors in the limbal stromal microenvironment. Dysfunction of the limbal stroma can lead to limbal stem cell deficiency/dysfunction (LSCD). Intuitively, damage to the stem cells, or its niche, will impact the normal functioning of the corneal surface. LSCD can be diffuse or focal and results in abnormal corneal healing and epithelialization, recurrent epithelial defects, ulceration, corneal neovascularization, stromal infiltration, scarring, and conjunctivalization. LSCD can be caused by a variety of inherited or acquired disorders. Acquired disorders associated with deficient or destroyed stem cells comprise the majority of cases seen clinically, including contact lens-induced keratopathy.
Key findings in LSCD include late fluorescein staining of the cornea and the presence of goblet cells on the corneal surface (identified by corneal impression cytology or corneal confocal examination).
Although uncommon, practitioners should consider LSCD in recalcitrant cases of keratopathy and ocular surface disease. CLS
Dr. Mastrota is a 1989 graduate of SUNY State College of Optometry. She is center director at the New York Office of Omni Eye Services and secretary of the new Ocular Surface Society of Optometry. She is also a consultant to Allergan, AMO, B&L, Inspire, and Cynacon OcuSoft.