


MYOPIA CONTROL STUDY
The SMART Study: Background, Rationale, and Baseline Results
This long-term longitudinal study aims to answer the question of whether ortho-k can control myopia.
By S. Barry Eiden, OD, FAAO; Robert L. Davis, OD, FAAO; Edward S. Bennett, OD, MSEd, FAAO; and Julie O. DeKinder, OD, FAAO
| Dr. Eiden is co-founder of EyeVis Eye and Vision Research Institute and president of a private group practice in Illinois. He has a financial interest in Alternative Vision Solutions, LLC, is a consultant or advisor to CIBA Vision, CooperVision, SynergEyes, Alcon, and SpecialEyes and has received research funds from Vistakon, CooperVision, and B&L. Dr. Davis is co-founder of EyeVis Eye and Vision Research Institute. He practices in a suburb outside Chicago. He is an advisor or consultant to CooperVision and SynergEyes, has received research funds from CooperVision and B&L, and has a proprietary interest in SpecialEyes and Alternative Vision Solutions. Dr. Bennett is an associate professor of optometry at the University of Missouri-St. Louis and is executive director of the GP Lens Institute. Dr. DeKinder is an assistant clinical professor at the University of Missouri-St. Louis College of Optometry. |
Myopia is the most common human eye disorder in the world and continues to represent a worldwide public health problem. Estimates indicate that its prevalence in the United States is 25 percent (Sperduto et al, 1983; Vitale et al, 2008; Wang et al, 1994; Katz et al, 1997; Goss and Winkler, 1983; Kempen et al, 2004). It is associated with an increased risk for visual loss, including accounting for 5.6 percent of blindness among U.S. schoolchildren (Tokoro, 1982). Myopia remains one of the most prevalent ocular disorders for which a uniformly acceptable solution has yet to be found.
There is particular interest in the correction of myopia in young people soon after its diagnosis to improve quality of life. About 15 percent of children become myopic between the ages of 6-to-14 years, with vision correction often necessary between 8-to-10 years of age.
The more important question for young people and their parents is: how can the growth of myopia be slowed down? Estimates indicate that slowing the progression of myopia in this 6- to 14-year-old age group could impact 40 million or more adults in the United States because of fewer ocular health risks with low (rather than high) myopic refractive error.
Background
Myopia Control Studies Myopia progression is primarily due to elongation of the axial length (AL). If myopia is to be controlled during its development, the correcting device must reduce the progression of eye growth. Walline et al (2008) found that over a three-year period, soft contact lenses did not have any significant effect on slowing AL progression in young lens wearers versus in spectacle-wearing young people.
Early studies found that progressive addition spectacle lenses and both PMMA and conventional GP contact lenses did result in some effect on the progression of myopia (Morrison, 1960; Stone, 1976; Perrigin et al, 1990; Khoo et al, 1999; Walline et al, 2004). However, all of these studies failed to find a clinically meaningful slowing of eye growth.
More recent studies have demonstrated very little difference between myopia increase in GP wearers versus spectacle-wearing and soft contact lens-wearing young people. In the Contact Lens and Myopia Progression (CLAMP) Study (Walline et al, 2004), although a greater increase in myopic refractive error occurred in the soft contact lens control group over a three-year period, much of this difference was attributed to corneal flattening from GP lens wear during the first year of the study. No difference in AL progression was noted between the two groups.
A More Promising Option One corrective treatment modality that has exhibited great potential in myopia management is orthokeratology, also known as corneal reshaping. In the last 20 years, this modality has experienced a rebirth due to the introduction of reverse geometry lens designs, which incorporate a steep reverse curve adjacent to the base curve radius as well as one-to-two alignment curves located between the reverse curve and a peripheral curve.
Recent surveys of contact lens prescribing habits have confirmed the increasing influence of orthokeratology. Although worldwide the use of GP lenses is decreasing, estimated at 9 percent of fits in 2008, ortho-k fits are approximately 1 percent of new fits or 11 percent of all GP fits.
Patient satisfaction with ortho-k has been confirmed through several quality of life survey studies. Ritchey et al (2005) found not only similar quality of life responses in most categories for ortho-k versus 30-day continuous wear silicone hydrogel lens wear, but also that the unaided high- and low-contrast vision of the ortho-k group was similar to the aided vision of the continuous wear group. For subjects wearing both daily wear disposable soft lenses and ortho-k, although the soft lens wearers achieved better visual acuity and less glare, slightly more than two-thirds (67.7 percent) preferred ortho-k at the conclusion of the study. These studies found that ortho-k subjects had fewer limitations on daily activities, reduced dependence on correction, and less lens-related symptoms. Also using a quality of life survey, Rah et al (2004) found no difference in results between overnight ortho-k and refractive surgery patients. This included comparing their perceptions about vision, activity limitations, dependence on correction, and satisfaction with correction.
Studying Ortho-k Effectiveness The most important question pertains to how much myopia is reduced with overnight retainer wear of ortho-k lenses and what improvement results in unaided visual acuity. The first studies to assess overnight ortho-k were limited to adult (18 years of age) subjects. The average amount of myopia reduction ranged from –1.76D to –3.33D, with the average final unaided acuity approximating 20/20 (6/6) (Swarbrick, 2006). The amount of average myopia reduction is somewhat misleading, however; if the higher myopia subjects (i.e., –2.75 to –4.50D) are separated from the lower myopia subjects (i.e., <–2.75D), then the average refractive error reduction is greater than –3.50D.
It is evident that much of the recent research in ortho-k has focused on young people, notably in the 8-to-15 age group. This age group in particular may derive several potential benefits from overnight ortho-k. Children of this age are very active and would benefit from not wearing spectacles or contact lenses for their athletic activities. Certainly the quality of life achieved from not wearing a correction during waking hours would be improved relative to depending upon spectacles or contact lenses for correction.
Several recent studies focused exclusively on young people have concluded that ortho-k has great promise as an effective method of myopia control. Also, the effects of ortho-k occur at a faster rate with young people than with adults. More important has been the effect on myopia progression as evidenced by changes in AL and vitreous chamber depth (VCD). Cho et al (2005) found an approximate twofold increase for spectacle wearers versus for ortho-k wearers in both AL (0.29mm for ortho-k versus 0.54mm for the spectacle-wearing control group) and VCD (0.23mm for the ortho-k group versus 0.48mm for the control group) over a two-year period for young people between the ages of 7 years and 12 years. Walline (2007) confirmed these results with the first-year results of the Corneal Reshaping and Yearly Observation of Nearsightedness (CRAYON) study in which daily wear of both conventional GP lenses and soft lenses resulted in an AL increase of 0.35mm whereas ortho-k wear resulted in AL growth of only 0.15mm.
However, these clinical studies have suffered from certain limitations including one or more of the following: small sample size, high dropout rate, very little — if any — evaluation of regression of refractive error change with lens removal, and limited study duration. The latter is particularly notable as the aforementioned studies had a duration of six-to-24 months, which is likely an insufficient time period to monitor long-term AL and VCD growth as well as such factors as stability of refractive error change, dropout rates, and complications.
Rationale
The aforementioned study limitations resulted in the development of the Stabilizing Myopia by Accelerating Reshaping Technique (SMART) study. The intent of the SMART investigation is to determine whether wearing corneal reshaping lenses on an overnight basis stops or slows the progression of myopia in children. The objective of this multicenter investigational protocol is to explore the myopia stabilization effects of wearing reverse geometry contact lenses and compare them to the controls (wearing daily wear soft contact lenses) as measured by change in refraction, AL, and VCD. This analysis aims to document anatomical changes that may be associated with increases in myopia as measured by AL and VCD, topography, endothelial cell count, intraocular pressure, and corneal thickness. During the five-year study follow-up period, this investigation will also compare the subjective aspects of vision and comfort between GP reverse geometry contact lens wearers and soft disposable contact lens wearers. This will be the first at large examination investigating the outcome analysis of a corneal reshaping technique.
The remainder of this article will review the protocol and goals of the SMART study.
Methods
Study Enrollment and Locations This study is being conducted in accordance with the guidelines provided by the Declaration of Helsinki and in adherence to the guidelines of the respective institutions conducting this study. The investigators/investigational sites include the following: Robert Davis, OD, FAAO (Davis Eye Care Associates, Oak Lawn, Ill.), and S. Barry Eiden, OD, FAAO (North Suburban Vision Consultant, Ltd., Deerfield, Ill.) as co-principal investigators; Michael Lipson, OD, FAAO (University of Michigan Department of Ophthalmology and Visual Sciences, East Lansing, Mich.); Bruce Koffler, MD (Lexington, Ky.); Lisa Wohl, MD (Bloomingdale, Ill.), Edward Bennett, OD, MSEd, FAAO (St. Louis, Mo.); P. Douglas Becherer, OD, FAAO (Belleville, Ill.); Robert Gerowitz, OD, FAAO (Palatine, Ill.); Cary Herzberg, OD, FAAO (Aurora, Ill.); and LaMar Zigler, OD, FAAO (Columbus, Ohio).
The study includes 162 treatment subjects (80 female, 82 male) fitted by the aforementioned 10 investigational sites to determine a reliable outcome analysis for patients fitted with the Boston Equalens II (Bausch & Lomb) GP contact lens polymer in an ortho-k fitting philosophy (Emerald Contact Lens for Overnight Orthokeratology, Euclid Systems Corporation). The net effect of this contact lens fitting philosophy is to change the corneal shape for the sole purpose of reducing the amount of myopia measured by conventional methods. One-hundred-and-five subjects (65 female, 40 male) serve as controls. These individuals were fitted with the PureVision (Bausch & Lomb) lens worn for daily wear use and monthly replacement.
The treatment group has a mean age of 11.1 years (ranging from 7-to-14 years); the control group has a mean age of 11.7 years (ranging from 7-to-15 years). Table 1 shows the entrance correction methods of the experimental and control groups at enrollment into the study. Figure 1 shows baseline manifest and cycloplegic refraction of the test and control groups, while Figure 2 shows corneal curvature, Figure 3 shows AL and VCD, and Figure 4 shows pachymetry.
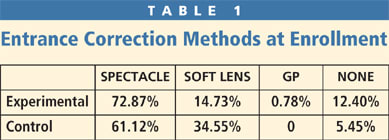
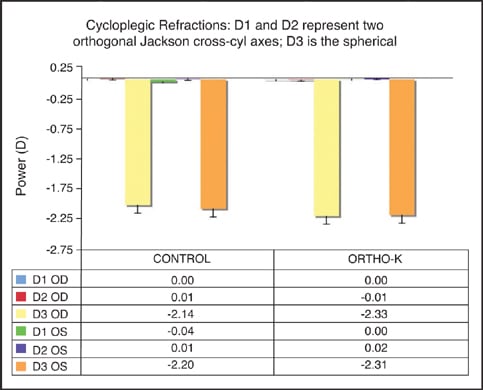
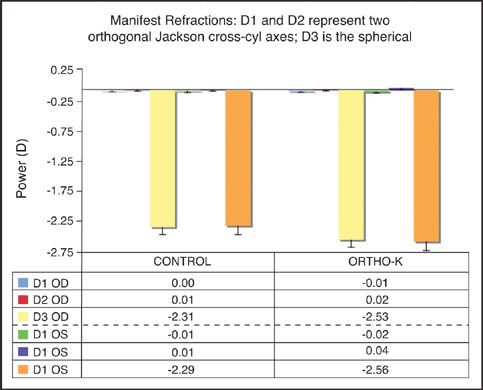
Figure 1. Baseline statistics for cycloplegic and manifest refraction.
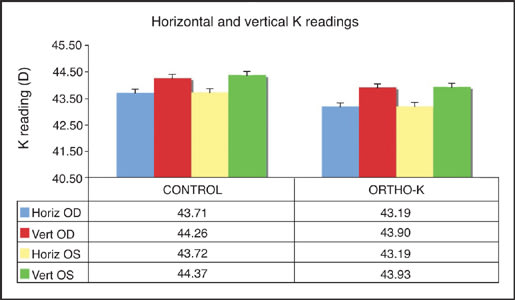
Figure 2. Baseline statistics for horizontal and vertical corneal curvature.
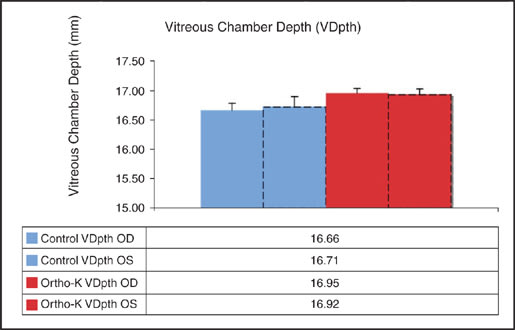
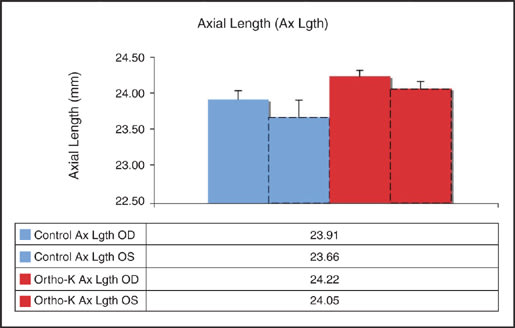
Figure 3. Baseline statistics for vitreous chamber depth and axial length.
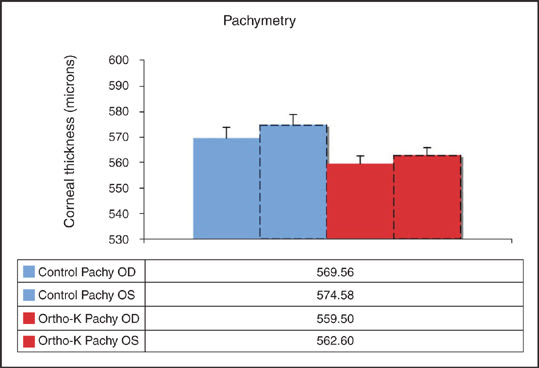
Figure 4. Baseline statistics for pachymetry.
Subject Selection (Inclusion/Exclusion Criteria) The investigators selected potential candidates without any requirements as to sex or occupation of the subjects or racial/ethnic/religious backgrounds. Subjects currently undergoing ortho-k or subjects previously successful or unsuccessful in daily or overnight ortho-k were not eligible for the study.
Inclusion Criteria
1. Refractive error, non-cycloplegic refraction: sphere powers from –0.75D to –5.00D, inclusive; cylinder powers up to –2.00DC in axes of 180 degrees ±20 degrees, all other axes up to –1.00DC.
2. Age: male or female subjects 7-to-14 years inclusive at baseline pre-treatment examination.
3. Contact lenses: subjects with previous or current contact lens wear could be included into the investigational study as long as they discontinued lens wear for a minimum of one month before the study. Subjects must exhibit refractive stability, confirmed by clinical records. If subjects wore rigid contact lenses, two central keratometry readings should not have differed by more than –0.50D in either meridian. The mires should be regular. No previous orthokeratology patient could be admitted into the investigational study.
4. Visual acuity: 20/25 or better, best-corrected in each eye.
5. Ocular health: must be free of eye disease and binocular vision problems (e.g., strabismus, amblyopia, oculomotor nerve palsies, corneal disease, etc.) that may affect vision or contact lens wear. Subjects must have normal healthy eyes with no evidence of lid infection or structural abnormality; a conjunctiva free of infection; a cornea clear and free of edema, scars, staining, vascularization, infiltrates, or opacities when examined by slit lamp biomicroscopy; and no evidence of iritis or uveitis (slit lamp findings of grade 0 or 1 could be admitted into the investigational study).
6. Systemic health: must be free of systemic disease that may affect vision or vision development (e.g., diabetes, Down syndrome, etc.). Subjects must have no history of allergies that would contraindicate solution use and/or "normal" contact lens wear.
7. Prescription and spectacles: subjects must have naturally occurring refractive myopia (range as listed previously) and refractive astigmatism (as listed previously) as determined by manifest refraction. The subjects must be wearing a single vision spectacle lens or no spectacle lens at all at the time of the baseline visit.
8. Medications: subjects must not be taking or must not anticipate taking drugs that might alter normal ocular physiology (e.g., eye drops containing ephedrine, phenylephrine, etc.), thereby affecting or interfering with successful contact lens wear.
9. Office visits: subjects must be willing to attend all scheduled office visits for the duration of the investigation.
Exclusion Criteria
1. Individuals participating in other clinical studies.
2. Individuals who have clinical signs of keratoconus or other corneal abnormalities.
3. Individuals who are taking or who plan to take medication that may cause dry eye (e.g., Accutane) or affect vision, corneal curvature, or healing (e.g., corticosteroids).
4. Individuals who have undergone intraocular or corneal surgery of any kind.
5. Individuals who have an allergy to any ingredient in the study lens care solutions.
6. Individuals who have corneas that demonstrate unstable central keratometry, irregular mires, or that show irregular corneal topography.
7. Females who were pregnant, breastfeeding, or who intended to become pregnant over the course of the study.
8. Individuals who do not meet the inclusion criteria.
9. Individuals who have any ocular structural abnormality or latent disease (e.g., herpes keratitis) that would contraindicate "normal" lens wear.
Examination Procedures The investigators examined subjects for eligibility at the baseline examination. Subject data was collected at the initial visit and will likewise be collected at all follow-up visits. At the dispensing visit, treatment subjects were given their contact lenses and taught how to apply, remove, and care for their lenses. The day after the first night of contact lens wear, investigators examined the treatment subjects within one hour of waking. At one week, two weeks, one month, three months, six months, one year and every six months thereafter, the treatment subjects were/will be evaluated, at minimum, eight hours after lens removal. Control subjects are evaluated following a minimum of four hours of lens wear. Both the test and control groups will be monitored for refractive changes at each visit. If a prescription change is discovered, the lens power change is provided.
Investigators are evaluating each subject for up to a five-year period. The timetable of patient visits was initiated after the investigator acknowledged that the lens specifications were appropriate. Each examination consists of the following procedures:
- Visual acuity (VA) Bailey-Lovie low- and high-contrast acuity charts: total letter count and test distance recorded on the case report form
- Corneal topography
- Refraction (manifest at each visit and cycloplegic annually)
- Slit lamp examination
- Endothelium cell count with specular microscopy: selected sites (Davis and Becherer)
- Contact lens comfort, handling, and wearing time questionnaire
- A-Scan measurements (AL, VCD)
a. Dilated fundus examination (annually)
b. Pachymetry (semi-annually)
c. Intraocular pressure (annually)
d. Keratometry
With treatment subjects, once a year the lenses will be removed and refractive, A-Scan, and keratometric/topographic readings will be analyzed for stabilization and progression. At yearly intervals, each subject will return their treatment lenses to the investigator to be replaced with soft lenses. Subjects will be monitored by refraction, topography, A-Scan, pachymetry, and keratometric readings every three days post discontinuation of ortho-k lens wear until two consecutive visits exhibit stabilized readings. The investigators will compare the readings to baseline to illustrate the net effect of the treatment procedure. After the data have been collected, patients will resume treatment in a new lens with the same specifications as the lens that was returned to the investigator. This procedure will continue each year that subjects are enrolled into the study.
The same data was collected with the control group. At yearly visits the control group is monitored by refraction, topography, A-Scan, pachymetry, and keratometric readings. The readings will be compared to baseline to illustrate the net effect of the control group.
If uncorrected vision was reduced during the initial treatment period, disposable soft contact lenses were provided or the investigational product was worn during daytime hours until adequate vision was achieved. This may have been necessary during the initial two-to-three weeks of the study while the treatment effect was stabilizing. Wear of soft contact lenses was temporary and used only when necessary.
Investigators provided Boston Conditioning Solution and Boston Cleaner (both Bausch & Lomb) to all treatment subjects in this study. If subjects show clinical signs or symptoms of solution allergies, an alternate solution regimen such as Optimum CDS Cleaning, Disinfecting and Storage Solution and Optimum CDS Extra Strength Cleaner (both Lobob Laboratories) will be dispensed. All control subjects were dispensed ReNu MultiPlus (B&L).
Preliminary Fitting Results for the Ortho-k Study Lenses
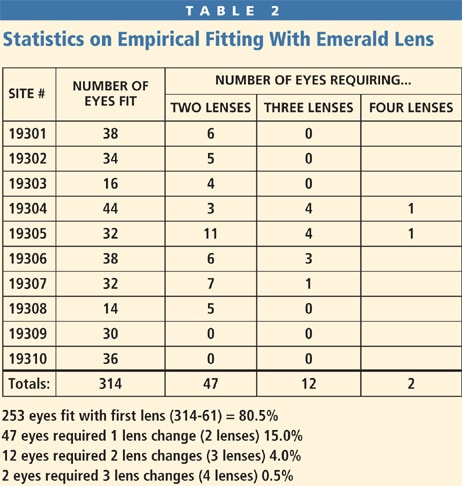
Of the 10 investigational sites, only two had previous experience in fitting Euclid Emerald corneal reshaping contact lenses. The only data investigators provided to Euclid to design the initial corneal reshaping lenses was manifest refraction, keratometric data, and corneal diameter. Based on this information the initial success of fitting was remarkably high. As shown in Table 2, 80.5 percent of eyes fit into ortho-k were successfully fit with the first lens. Furthermore, 95.5 percent of orthokeratology-wearing eyes were successfully fit with, at most, one lens change. Success was defined as patient satisfaction with the lens and 20/25 or better unaided visual acuity.
Discussion
The importance of the SMART study is, in part, its longitudinal nature. Evaluating young people over this long of a time period allows for assessment of such factors as regression over time, AL and VCD change, rate of contact lens loss, dropout rates, corneal thickness change, endothelial cell change, and adverse events, and the results can be compared with those of a control group of individuals wearing a contemporary silicone hydrogel contact lens material. Therefore, the investigators can assess the effect of myopia stabilization with overnight corneal reshaping on an annual basis through the five-year length of the study.
The assessment of long-term adverse events is especially important. In particular, the frequency of microbial keratitis with a large subject population over a five-year time period will be important to determine. The SMART study should help determine the safety level of overnight orthokeratology lens wear among young people in the United States.
The introduction of four- and five-zone reverse geometry ortho-k contact lens designs in the 1990s has also resulted in the likelihood that patients can achieve success with their first pair of contact lenses as opposed to reducing myopia to a desired level via a series of progressively flatter lenses. Chan et al (2008) reported a first-fit ortho-k success rate of 73.5 percent, with 16 percent requiring two pairs for a successful fit and 7.4 percent needing three pairs. With the large subject sample in the SMART study, obtaining more than 80 percent first-fit success and more than 95 percent with up to one exchange could make a strong argument for the ease of fit as well as the level of patient satisfaction that is obtainable with this modality.
Conclusions
It is evident that interest in overnight ortho-k for young people is growing based upon the numerous clinical studies performed in recent years. However, these studies have only evaluated subjects over a period of no more than two years and often for only six months or less. In addition, the need for a large multicenter longitudinal study that evaluates eye growth, effects of regression over time, ocular health, and corneal thickness change is very evident. The SMART study has the potential to be a definitive study on the safety and efficacy of overnight orthokeratology and the ability of this treatment modality to control myopia progression. CLS
The authors would like to acknowledge Bausch & Lomb for sponsoring the study, Euclid Systems Corporation for providing lenses used in this study, and information provided by Natalie Cogswell, the SMART Study coordinator, and Caroline Blackie, the SMART Study statistician.
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #167.