


research review
Challenging Traditional Theories in Microbial Keratitis
BY LORETTA B. SZCZOTKA-FLYNN, OD, MS, FAAO
Rarely, someone comes along in the contact lens field who blends in-depth contact lens clinical experience with extensive basic science training and knowledge. Dr. Suzanne (Suzi) Fleiszig is one such individual. Dr. Fleiszig completed her training in optometry at the University of Melbourne (Department of Optometry) in Australia where she also completed her PhD degree.
She moved to the United States in 1991 where she accepted a postdoctoral fellowship at Harvard University. She then completed three years of postdoctoral study in infectious diseases at the Department of Medicine at Harvard Medical School. During that time she was awarded a Fight for Sight Postdoctoral Fellowship by the National Society to Prevent Blindness and a C.J. Martin Postdoctoral Fellowship by the Australian Government. Dr. Fleiszig was then promoted to the faculty at Harvard Medical School.
Currently a professor of optometry at the University of California, Berkeley (UCB), Dr. Fleiszig also holds appointments in the Microbiology, Vision Science, Infectious Diseases & Immunity, and Health & Medical Sciences Programs at UCB, reflecting the interdisciplinary nature of her research. Dr. Fleiszig is currently the President of the International Society for Contact Lens Research, Chair of the Immunology and Microbiology Section of the Association for Research in Vision and Ophthalmology (ARVO), the Chair of Division D (Bacteria of Medical Importance) of the American Society for Microbiology, and she is a permanent member of the Anterior Eye Disease (AED) Study Section for the NIH.
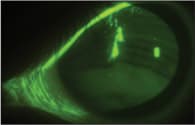
Figure 1. A deep corneal abrasion.
Dr. Fleiszig was honored by the American Academy of Optometry in 1997 with the Borish Award and in 2005 with the Glenn A. Fry award.
Researching Infectious Keratitis
Research in Dr. Fleiszig's laboratory focuses on the pathogenesis of bacterial infections of the cornea, most often Pseudomonas aeruginosa infections. The principal aim of her research is to determine why patients who wear contact lenses are prone to infectious keratitis.
Dr. Fleiszig's work over the years has opened up new doors and challenged traditional thinking in contact lens-induced microbial keratitis. In a normal, healthy ocular surface, bacterial inoculation does not usually result in infection. In fact, her laboratory has reported that normal, healthy eyes clear viable bacteria within a few hours, likely from the involvement of preformed innate immune defense mechanisms (Mun et al, 2009). It is widely believed that infection is prevented because bacteria cannot adhere to the cornea or penetrate to the stroma unless the epithelial barrier is grossly damaged, as it is in the deep corneal abrasion shown in Figure 1.
However, Dr. Fleiszig's research team has shown that P. aeruginosa can be present in one of two strains and can adhere to an uninjured cornea. One strain can enter corneal cells and replicate inside them, the other type is cytotoxic and can quickly kill corneal cells.
At the last two annual ARVO meetings, her laboratory has shed more light on the fact that breaching the epithelial barrier may not be required to cause corneal infection.
Disrupted Versus Intact Corneal Epithelium
At the 2008 ARVO meeting, Dr. Fleiszig's research team reported on a rat contact lens model in which they either did or did not disrupt the epithelium by blotting with tissue paper. Low-Dk contact lenses were then soaked in high levels of P. aeruginosa and placed on the corneas for two hours. The results showed that it took five-to-14 days for the disrupted rat corneas to develop infection after blotting and the bacterial inoculation procedure. The researchers concluded that epithelial disruption does not initially enable infection, even when bacteria are purposely added with contact lens wear. However, bacteria can then survive at the ocular surface after continued contact lens wear to ultimately cause disease within one-to-two weeks.
Additionally, in a related study using a similar blotting/inoculation mouse model, the corneal epithelium remained several cell layers thick after blotting. Although blotted eyes stained with fluorescein and showed increased susceptibility to bacterial attachment, blotting alone did not make corneas susceptible to bacterial penetration beyond the superficial epithelium, nor did it produce susceptibility to keratitis.
In fact, the researchers also showed that a single high-inoculum (109 colony forming units) of P. aeruginosa administered when fitting a low-Dk contact lens enabled corneal infection in rats. Disease occurred within five-to-14 days and did not require other manipulations to the cornea.
Lastly, at the ARVO meeting in 2009, Dr. Fleiszig's laboratory produced a rat contact lens model of microbially induced corneal inflammation in which the researchers did not damage the corneal epithelium and they used lower inocula to mimic the clinical environment. In these studies, low-Dk hydrogel contact lenses were soaked for 24 hours in a minimal medium inoculated with 103 cfu/ml of P. aeruginosa. Once corneal inflammation was noted, the researchers removed the contact lenses and then transferred them to the eyes of naive rats. All eyes wearing contaminated contact lenses developed corneal disease within three-to-14 days. However, eyes wearing contact lenses transferred from infected animals also became infected, often much more quickly such as within 24 hours. This rapid infection was associated with classical bacterial biofilms that had formed in vivo on the posterior, but not the anterior, contact lens surfaces as confirmed by confocal microscopy.
The researchers concluded that a single bacterial inoculum placed on the intact rat cornea with a contact lens enabled infection regardless of whether a high-or low-dose inoculum was used. The bacteria that persisted beneath the contact lens formed biofilms on the posterior contact lens surface and ultimately caused disease within one or two weeks. The biofilms formed on the contact lenses in vivo and became extremely virulent, able to induce infection after only one day.
Time for a New Focus
As noted in my May Research Review column titled “Biofilms and Contact Lenses,“ biofilms are communities of organisms that create their own complex environment on a surface where they communicate, seek nutrients, and excrete substances to shield and protect themselves. They become extremely resistant to disinfectants and to the host immune system. Previous studies have shown that contact lens biofilms can form on lenses while being worn by human patients, and this data confirms that the same occurs in the rat contact lens model. These data suggest that bacteria can adapt to the in vivo environment and create a highly resistant and pathogenic biofilm that likely contributes to the pathogenesis of contact lens-related keratitis on uninjured corneas.
The type of work performed in Dr. Fleiszig's laboratory suggests that a virulent organism can override the normal host defenses, including an intact epithelium. This makes me think that we should shift the debate about subtle corneal injury such as superficial solution-induced corneal staining to mechanisms for preventing the attachment of virulent organisms and biofilm formation. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #166.
Dr. Szczotka-Flynn is an associate professor at the Case Western Reserve University Dept. of Ophthalmology & Visual Sciences and is director of the Contact Lens Service at University Hospitals Case Medical Center. She has received research funding from CIBA, Vistakon, Alcon, and CooperVision.