


FITTING HYBRID LENSES
Hybrid Contact Lens Management
This fitting and patient selection approach can increase your success with hybrid lens fitting.
By Robert Davis, OD, FAAO, & S. Barry Eiden, OD, FAAO

Dr. Davis is co-founder of EyeVis Eye and Vision Research Institute. He practices in a suburb outside Chicago. He is an advisor or consultant to CooperVision and SynergEyes, has received research funds from CooperVision and B+L, and has a proprietary interest in SpecialEyes and Alternative Vision Solutions. |

Dr. Eiden, co-founder of EyeVis Eye and Vision Research Institute, is president of a private group practice in Illinois. He has a financial interest in Alternative Vision Solutions, LLC, is a consultant or advisor to Ciba Vision, CooperVision, SynergEyes, Alcon, and SpecialEyes, and has received research funds from Vistakon, CooperVision, and B+L. |
Success in contact lens wear is predicated upon achieving vision goals, lens wearing comfort, and appropriate ocular health and physiological response. It is well accepted that in most situations, a rigid contact lens provides superior vision quality in comparison to soft contact lenses. However, rigid lenses still suffer from inferior initial comfort compared to soft lenses when fit on non-adapted eyes. In addition, a soft contact lens will tend to center more precisely over the cornea compared to a rigid lens, especially in cases of corneal surface irregularity. Initial comfort limitations of rigid lenses have resulted in soft contact lens fitting dominating the marketplace.
The concept of combining rigid lens optics with soft lens comfort and positioning was initially attempted through fitting piggyback lens systems (a rigid lens fit over the surface of a soft lens). While still highly effective, piggyback lens fitting suffers from the inconvenience of requiring patients to manipulate and care for two separate lenses per eye. The “ultimate” contact lens would be a single lens with the advantages of both a rigid and a soft contact lens. Thus, the concept of a “hybrid” contact lens was conceived.
Hybrid Lens History
The first hybrid contact lens was introduced in 1983 as the Saturn II design by Precision-Cosmet. Due to design performance issues, the lens was re-designed and re-introduced by Sola/Barnes-Hind Inc. laboratories as the SoftPerm lens in 1985. The initial indications for this hybrid contact lens included improving performance and comfort for the fitting of irregular corneas in comparison to rigid contact lenses. In addition, it was designed for managing regular astigmatism and spherical refractive error for cases in which rigid contact lens adaptation could not be achieved.
Problems with the SoftPerm hybrid contact lens included low oxygen transmission of both the rigid and soft sections, lens breakage and splitting at the rigid/soft interface, lens adherence, and flexure of the rigid lens portion. Although currently still available from Ciba Vision, the SoftPerm lens is used by few practitioners typically for lens replacement for the limited number of patients who were initially successful with the lens.
In 2001, Quarter Lambda Technologies (later to become SynergEyes, Inc.) began research and development of a new hybrid contact lens that ultimately received FDA approval in 2005 as the SynergEyes hybrid contact lens. The SynergEyes hybrid lens differed from the SoftPerm design in the use of a high-Dk central GP material (Paragon HDS 100, Paragon Vision Sciences) and the development of a “Hyperbond” junction between the rigid and soft portions of the lens that significantly reduced the incidence of splitting between the two sections (common to the SoftPerm). The soft skirt portion is a 27-percent water, nonionic, group 1 material with a permeability of 9.3 X 10−11. In addition, the SynergEyes lens is available with adjustable soft skirt curves as well as multiple rigid base curves, thus allowing for more precise control of lens fitting characteristics.
The company initially developed and distributed four design variations of its hybrid lens technologies including the “A” design for fitting standard corneas, the “KC” design for fitting some cases of keratoconus and other highly prolate corneas, the “PS” design for fitting post-surgical corneas and other eyes that have oblate topographies, and the SynergEyes Multifocal design for fitting presbyopic eyes. Most recently, SynergEyes introduced the ClearKone design, which is intended to fit irregular corneas. It has an advantage over the KC design in cases of decentered cones, which tend to result in lens bearing or seal-off when fit with the KC lens design. The ClearKone is fit with a vaulting method that allows for clearance over the apex of the cone. The reverse curves in the lens design appropriately return the lens onto the cornea for adequate tear flow.
Standard Fitting Methods
For purposes of simplicity, we will limit our discussion in this article to fitting the standard SynergEyes A and Multifocal designs, both of which have similar geometries and fitting characteristics. However, basic principles of a successful hybrid lens fit can be generalized to all of the lens designs.
SynergEyes suggests that the A and Multifocal lenses can be fit empirically based on keratometric, refractive, and corneal diameter data. It is, however, indicated that diagnostic lens fitting provides more accurate information as well as practitioner and patient feedback and increases the success rate of first lens fitting. Both the A and Multifocal lens designs have available diagnostic lens fitting sets.
Optimal lens fitting characteristics according to the manufacturer will demonstrate:
- Apical clearance over the entire rigid portion of the lens.
- Absence of large bubbles under any portion of the lens.
- Alignment of the soft skirt over the peripheral cornea and sclera.
- Lack of soft skirt edge gape or “fluting” (Figure 1) nor any scleral impingement.
- Adequate lens movement (described as “slight movement with blink”).
The company suggests that for normal corneas with up to 2.00D of corneal toricity, a diagnostic SynergEyes lens with a base curve of 1D to 1.5D (0.2mm to 0.3mm) steeper than the flat keratometric meridian should be initially selected. For a cornea that has greater than 2.00D of corneal toricity, two-thirds of the difference should be added to the flat keratometric meridian. The company suggests that for lenses exhibiting inadequate movement, initially confirm the central clearance and if inadequate, select a steeper base curve. If inadequate movement occurs when there is adequate central clearance, a soft skirt of steeper curvature should be selected. Soft skirt fluting should be addressed with a steeper skirt curve, and scleral impingement should be addressed with a flatter skirt curve.

Figure 1. SynergEyes design with fluting.
An Alternative Fitting Approach
We have found that following the standard fitting methods may result in outcomes that are less than optimal. The most common problem reported by practitioners is that the SynergEyes hybrid contact lens tends to “tighten up,” seal-off (Figure 2), and result in an inflammatory ocular response with significant discomfort. An alternative fitting approach that we have developed based on extensive clinical experience has resulted in higher fitting success rates with SynergEyes lenses in our practices.
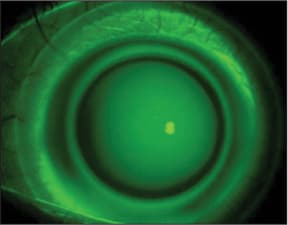
Figure 2. Inadequate flow of tears (seal-off).
Proper base curve and skirt curve selection will address the seal-off problem in the vast majority of cases. Selecting the wrong base curve or skirt curve will result in the patient returning to the office with discomfort and a red eye after a few hours of lens wear. This is not the time to give up on this lens design. The feedback from the corneal response is your chance to right the wrong. A key in achieving a proper fit is to allow the lens (diagnostic or dispensing) to settle on the eye for at least 10 minutes before evaluating the fit, especially in terms of lens movement. We feel that greater lens movement than what the company suggests is a critical element for success. We require that SynergEyes lenses move at least 0.5mm with the blink after they have been worn for longer than 10 minutes.
Base Curve Selection Based on traditional contact lens fitting techniques, a reasonable approach is to take the keratometric values and use the midpoint for the initial base curve selection. If the resultant radius is between available base curves, round to the nearest steeper base curve. The lens needs to slightly vault the cornea to provide a reservoir of tears beneath the lens. Fitting the lens flat will cause inadequate clearance between the cornea and the lens, resulting in bearing and chafing (Figure 3). Fitting a lens too steep will result in central bubble formation and potential seal-off of the periphery of the rigid portion of the lens (Figure 4). Placing high-molecular-weight fluorescein in the bowl of the lens prior to application allows you to assess lens-to-cornea geometries; we have found that the fluorescein pattern often confirms our observations when we correctly select the appropriate base curve utilizing our fitting method. Inappropriate fluorescein patterns typically indicate that our measurements of corneal curvature were erroneous and that remeasurement is in order.
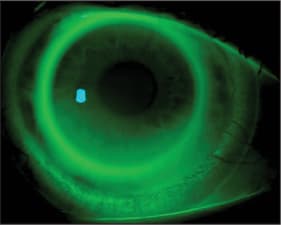
Figure 3. Flat fitting central curve (bearing).
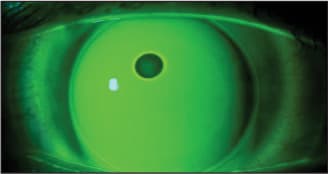
Figure 4. Steep fitting lens with seal-off (air bubble trapped).
For a spherical cornea, fitting the lens 0.50D steeper than the keratometric curve provides enough clearance for tears to reside under the central portion of the lens (Figure 5). For example, for a spherical eye with K readings of 43.00 / 43.00 we will select a lens 0.50D steeper (43.50D or 7.76mm), which results in a SynergEyes base curve of 7.70mm. Application of this base curve selection method (selecting a base curve 0.50D steeper than the flat K) is indicated for corneas that are spherical or mildly toric (up to 0.87D of toricity).
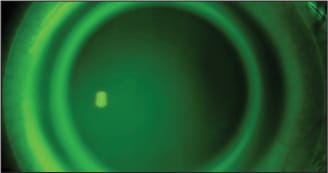
Figure 5. Properly fit SynergEyes lens. Notice the flow of tears.
Evaluate a more highly toric cornea in the same way. After the midpoint of keratometric values is calculated, select a base curve that matches this value. If this value falls between available base curves, select the next steeper base curve. For example, for a toric cornea whose measurements are 43.00D by 46.00D, it is impossible to find a base curve that will fit parallel to both curves unless we use a back-surface toric design (which is not currently available). So the idea is to have the lens create a “teeter-totter” effect on the cornea, slightly rocking back and forth on the corneal apex to create a flow of tears. The mid-K value is 44.50D (7.58mm) and the closest available base curve that is equal to or steeper than this value is 7.50mm.
Although the suggested method for base curve selection typically works for the majority of cases, occasionally we experience situations in which we have to modify our initial lens selections. If we use a base curve that is steeper than the midpoint K value, there's risk of corneal molding from the lens squeezing the periphery, causing the central K to steepen. As an example, we had a patient whose K values of 44.12 X 44.87 resulted in a calculated base curve of 44.62D (7.56mm). We selected a 7.50mm base curve as the best-fit lens. After two months of wear, the patient started becoming photophobic and developed central superficial punctate keratitis. The difference map (Figure 6) illustrates corneal steepening caused by the lens fitting steep. We ordered a new lens with a base curve of 7.60mm, which relieved all of the patient's symptoms and returned the cornea to the pre-fit topography (Figure 7). This example illustrates the importance of appropriate aftercare, differential diagnosis, and management.
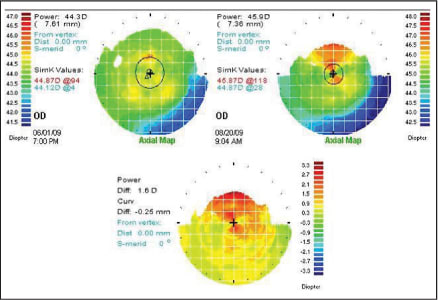
Figure 6. Difference map showing induced corneal steepening from a relatively steep SynergEyes lens fit.
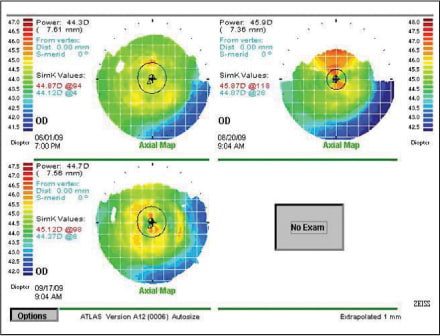
Figure 7. Initial topography (top left), topography with a 7.50mm base curve (top right), and with 7.60mm base curve (bottom).
Skirt Curve Selection Proper skirt curve selection also can significantly influence the overall lens fit. The skirt curve is analogous to the wings of an airplane creating lift. The available skirt curve options are either 1.0mm or 1.3mm flatter than the central curve. If the skirt is too steep, the lens will tighten significantly, creating scleral impingement and lens seal-off. When the skirt curve is selected appropriately, the lens design will ride under a stream of tears. We have found success by always selecting the flatter skirt curve unless fluting is observed (Figure 8). However, you have to be careful with your initial observations because occasionally this fluting can resolve after 10 minutes of wear. If you are impatient and select the steeper skirt curve, do not be surprised if at the one-week follow-up visit your patient exhibits seal-off and a red eye.
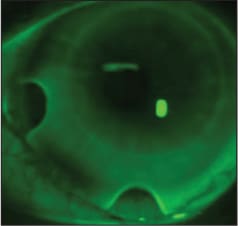
Figure 8. Flat skirt curve resulting in fluting.
A Side by Side Comparison If we compare our suggested fitting methodology to the standard fitting method (Table 1), we see certain significant differences. In terms of base curve selection, we realize that in some cases we will fit flatter, in other cases steeper, and occasionally the same as the standard fitting method.
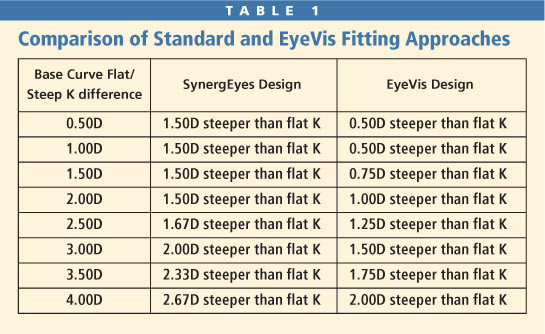
For the soft skirt curve selection, our approach is to fit the flattest skirt curve that avoids edge fluting. The standard fitting approach tends to favor steeper skirt curve fitting. Finally, in terms of movement, our technique suggests the importance of a greater degree of movement versus the standard fitting approach (0.5mm or more versus “slight movement”).
Patient Selection and Management
Additionally, the incorporation of basic management strategies has allowed us to develop a patient selection procedure that also increases success with SynergEyes lenses. Once you have achieved an appropriate physical lens fit (base curve and skirt curve) and have conducted an over-refraction, check the visual acuity, vision quality, and comfort response from the patient. If any of these important criteria are not to the patients liking, it is time to terminate the fitting process and explore other contact lens and vision correction options. Ask patients whether they would find the vision quality provided with the over-refraction and the comfort while wearing the lens to be adequate and acceptable for longer-term wear. If the response is positive, move forward. If negative on either level, terminate the SynergEyes lens fitting. If you try to encourage patients by suggesting that it takes time to adapt to either the vision quality or comfort, you will be looking at using the return policy in weeks to come. With this lens, what you see is what you get; the fit and vision rarely change over time.
Other SynergEyes Hybrid Lens Considerations
Lens replacement strategies for SynergEyes offer the option of replacing lenses either once a year or every six months. Most patients who care for the hybrid lenses appropriately will find that they last about a year with normal handling. The significantly increased cost of replacing these contact lenses every six months can dramatically reduce the potential patient pool.
If a patient is determined to pursue six-month lens replacement, we typically suggest the use of either Aquify or Clear Care (both Ciba Vision) cleaning and disinfection regimens. Eiden and Davis (2010) reported on 31 patients completing a care system response study with SynergEyes A lenses. Subjects selected Clear Care as the best solution for cleaning, disinfecting, and comfort, although patients preferred the Aquify system in a forced-choice scenario due to its ease of use. We suggest that patients who choose the yearly lens replacement schedule use Clear Care because of its superior efficacy as documented in this study.
A Problem-Solving Lens Modality
The SynergEyes family of hybrid lenses offers an opportunity to solve problems related to traditional soft and GP lens wear that were impossible to correct in the past. The SynergEyes contact lens design may improve vision and comfort when soft and GP lenses fail. Lipson and Musch (2007) demonstrated in their quality of life survey that SynergEyes offered improved vision when compared to a soft toric contact lens modality. Of the previous GP lens wearers in the study, 71 percent preferred the SynergEyes lens for comfort.
Once you understand the fitting system, you realize that the fitting process is similar to that of other GP contact lens designs. The rigid portion is an 8.5mm lens design with a 7.8mm optic zone. It delivers pristine optics and behaves like a rigid lens, conforming to all of the same rules. The soft portion allows the edges to fit under the upper and lower lids for improved comfort and minimal lid interaction, similar to any other soft lens. Fitting the base curve to allow for central clearance and the skirt curve for alignment with appropriate tear flow will result in a lens fit that demonstrates optimal movement with blinking and that avoids the pitfalls of lens tightening and secondary inflammatory response.
You may find that patient acceptance will be high because you've solved the contact lens problems that your patients have been complaining about for years. Remember not to force the issue and to partner with your patients to find a solution that satisfies their expectations. It starts when you enter the examination room and ends when your patient walks out of your office feeling comfortable and able to see better than ever before. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #173.