


MICROBIAL KERATITIS
A Closer Look at Microbial Keratitis
A guide to the signs, symptoms, and management strategies of this potentially sight-threatening condition.
By Aaron B. Zimmerman, OD, MS, FAAO, & Jason J. Nichols, OD, MPH, PhD, FAAO

Dr. Zimmerman is an assistant clinical professor of optometry at The Ohio University College of Optometry and associate chief of the contact lens clinic. He can be reached at azimmerman@optometry.osu.edu. 
Dr. Nichols is an assistant professor of optometry and vision science at The Ohio State University College of Optometry. He has received research funding from Alcon, Ciba Vision, and Vistakon. |
Microbial keratitis (MK) is a non-specific term collectively used to describe various types of corneal infections. More often than not, MK is used to describe bacterial keratitis because the other types of keratitis are specified as Acanthamoeba, fungal, or viral. Any type of keratitis has the potential to be visually devastating, in some cases necessitating penetrating keratoplasty or, rarely, enucleation (Kaye et al 2010).
Incidence rates of fungal keratitis and Acanthamoeba keratitis are difficult to determine because of the extremely low rates of infection, but contact lens wear increases the risk (Dart et al, 2009) (Ku et al, 2009). Although both types of infections experienced a temporary and very small spike in the last few years secondary to contact lens and solution problems, the number of cases of these disorders remains very small (Chang et al, 2006). Bacterial keratitis, while rare, is much more common than are Acanthamoeba and fungal keratitis and has been thoroughly investigated for more than 20 years (Poggio, 1989) (Stapleton et al, 2008).
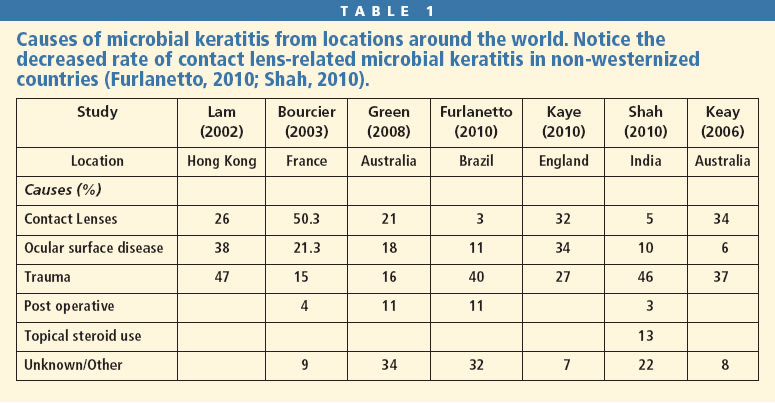
Non-contact lens wearers who have healthy ocular surfaces generally do not contract MK, so it is clinically thought that the normal physiology of the anterior ocular surface must be compromised in some way for this condition to occur. The primary causes of bacterial keratitis are contact lens wear, trauma, and ocular surface disease, with lens wear being the leading cause in westernized countries and trauma and ocular surface disease the leading causes in non-westernized countries (Lam et al, 2002; Bourcier et al, 2003; Green et al, 2008; Furlanetto et al, 2010; Kaye et al, 2010; Shah et al, 2010; Keay et al, 2006) (Table 1).
Incidence of Lens-Related Microbial Keratitis
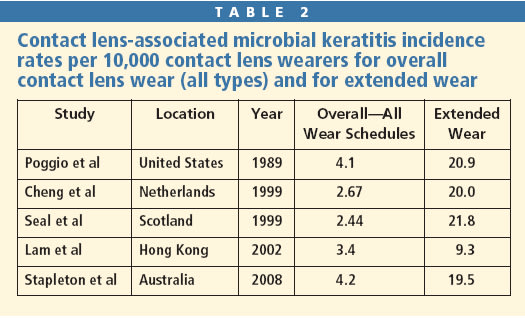
The first major publications regarding incidence and relative risk of contact lens-related MK appeared in 1989 (Poggio 1989; Schein 1989). They found that the incidence of MK was 4.1 per 10,000 for soft contact lens daily wear patients. For extended wear patients, the rate increased nearly five-fold to 20.9 per 10,000. Studies have since been performed in the Netherlands, Scotland, Hong Kong, and Australia (Cheng et al, 1999; Seal et al, 1999; Lam et al, 2002; Stapleton et al, 2008) (Table 2). The most recent study evaluating the incidence of MK among contact lens wearers was performed in Australia, and their incidence findings were nearly identical to those of Schein's study in 1989.
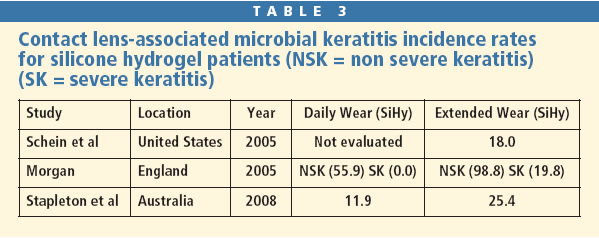
The Australia study evaluated the rate of MK associated with the use of hydrogel and silicone hydrogel (SiHy) contact lenses and showed that the rate of MK among SiHy lens wearers was actually higher for daily wear (11.9 per 10,000) and for extended wear (25.4 per 10,000). Schein specifically evaluated the incidence rate of MK with 30-day continuous wear silicone hydrogels and found a rate of 18 per 10,000—nearly identical to the rate of MK with extended wear of traditional hydrogels (Schein et al, 2005) (Table 3). Because silicone hydrogels provide increased oxygen permeability, many practitioners would previously have predicted a decrease in the rate of MK (Brennen et al, 1997). This clearly has not been the case, although the severity of the MK may be slightly reduced with silicone hydrogels (Keay et al, 2007).
The incidence rates of MK among individual lens modalities do differ. Gas permeable (GP) lenses are associated with the lowest incidence rate (~1.2 per 10,000), which may result from greater tear exchange that flushes both microbes and other mediators from behind the back surface of the lens (Ni et al, 2005; Fleiszig and Evans, 2010).
The incidence rate of MK associated with orthokeratology has been estimated at 7.7 per 10,000 (Bullimore, 2009). These infections certainly do occur, and many cases occurred several years ago in Asia (Watt and Swarbrick, 2005; Watt and Swarbrick, 2007). There was also a higher rate of Acanthamoeba keratitis associated with orthokeratology in Asia, which may have resulted from formerly poor contact lens regulation in China (Watt and Swarbrick, 2005). Although MK is rare, it is important for practitioners to educate their patients on the possible risks as well as encourage them to eliminate the use of tap water when rinsing their lenses (Watt and Swarbrick, 2007; Shehadeh-Masha'our et al, 2009).
Daily disposable lenses provide patients with a fresh lens each day and essentially eliminate the need for contact lens solutions and storage cases. A recent study evaluating patient compliance showed that daily disposable wearers in the United States and Canada have a compliance rate near 90 percent, which is the highest rate of all lens modalities (Dumbleton et al, 2010). Although daily disposable wearers are very compliant and these lenses eliminate the risk of contamination from solutions or cases, MK still occurs at a rate of approximately 2.0 per 10,000 (Stapleton et al, 2008). Daily disposables have the lowest risk of severe keratitis, defined as greater than two lines of vision loss, of all modalities.
Risk Factors
As mentioned previously, one of the greatest risk factors for MK is contact lens wear, which is responsible for 20 percent to 50 percent of all MK cases. Some contact lens-related risk factors are modifiable and are related to wear schedules, hygiene, habits, and health (Stapleton et al, 2007). Other risk factors are non-modifiable such as age, gender, socioeconomic status, time of year, and how long an individual has worn lenses. Practitioners should be aware of these risks, but with the knowledge that they are simply uncontrollable.
The modifiable risk factor associated with the highest risk is extended wear (Schein et al, 2005; Stapleton et al, 2008). Occasional overnight wear is not associated with rates as high as that of extended wear, but it is clear that this increases risk of MK. MK risk may be increased for vacationing contact lens wearers, which is most likely due to a change in wear and care habits that may include poor hygiene, occasional overnight wear, and swimming while wearing lenses. If overnight wear was minimized, the number of lens-related MK cases would certainly decrease.
Hygiene also tends to play a role in MK as unwashed hands may significantly contaminate lenses (Gromacki 2009). Nearly 35 percent of individuals do not wash their hands prior to applying their contact lenses, and even when hands are washed, many key areas are not appropriately cleaned. Although this seems intuitive, many people are ineffective at cleaning their hands, so proper instruction on hygiene may reduce the risk of MK.
Case hygiene should also be classified as a modifiable risk factor because patients easily have access to new cases at grocery stores, pharmacies, and large department stores. A recent study evaluated the microbial contamination of used contact lens cases from two subject samples (Wu et al, 2010). One group consisted of students at a university and the other came from the general contact lens-wearing population. All subjects at the time were free of complications. Participants placed their current case in a plastic bag and mailed it to the investigators who then sampled the inferior and superior portions of the used lens cases. Fifty-eight percent of the cases from each group were contaminated. The most common pathogens found were coagulase-negative Staphylococci, Bacillus, and fungi. A few cases tested positive for Pseudomonas, which was found near the top of each case. The Pseudomonas species are strict aerobes and therefore were found above the solution fill line. The investigators also found that cases less than nine months old had significantly less contamination compared to older cases. The authors support the United States Department of Health and Human Services recommendation for case replacement every three to six months.
Smoking has been implicated as a risk factor for MK for more than 20 years (Schein, 1989; Lam et al, 2002; Stapleton et al, 2008). In the Australia surveillance study, smoking increased the risk of MK by nearly three-fold. The chemicals that smoking releases into the ambient air are suspected to be toxic to the corneal epithelium, therefore damaging one of the physiologic barriers to infection. Swimming while wearing contact lenses, although not commonly found in the literature, also tends to be associated with an increased risk of MK (Whiting et al, 2004). Encourage patients to discard lenses after wearing them while swimming, particularly in a lake, river, or ocean, and certainly instruct them to not wear such lenses overnight. For individuals who swim on a daily basis, daily disposable lenses, while not perfect, are a good option.
Another risk factor is online purchasing of contact lenses, which creates a disconnect in the practitioner-patient relationship. The risk is nearly five times higher compared to those who order their lenses through their practitioner (Stapleton et al, 2008). This may reflect a perception by patients that contact lenses are not medical devices. This is magnified by the recent decision in British Columbia that allows individuals to order contact lenses without a prescription, which may increase the incidence of MK in that region (Hoster, 2010). We can certainly speculate that an individual who has never had a contact lens fit properly assessed and has never received proper instruction on hygiene, replacement schedules, and application and removal will be at a much higher risk of contracting MK.
Pathogenesis
The pathogenesis of MK has been extensively investigated for more than two decades, and the exact mechanism is still not fully understood (Fleiszig, 2006; Fleiszig and Evans, 2010). For a corneal infection to occur, the infecting organism must be capable of penetrating the natural defense mechanisms of the ocular surface. These mechanisms include the five to seven layers of the epithelium, the tear film, and the lids and their mechanical wiping of the surface, as well as the basal lamina.
The epithelium protects itself passively with tight junctions between cells and actively by releasing some factors that directly damage bacteria and others that chemotactically recruit immune cells. The tear film contains mucin, surfactant D, and IgA, which may all play a role in preventing a corneal infection. The lids mechanically remove debris from the ocular surface and therefore can help reduce the risk of infection. The basal lamina serves as a physical barrier to any bacteria that penetrates through the corneal epithelium (Alarcon et al, 2009). If the basal lamina is compromised secondary to trauma, the cornea is much more susceptible to infection (Fleiszig, 2006; Abrams, 2000)
The current model on the pathogenesis of an infection is structured based on knowledge about the defense mechanisms (Fleiszig, 2010). When an infection occurs, bacteria penetrate through the epithelium and basal lamina and ultimately end up in the anterior corneal stroma, causing significant inflammation. Previous studies have shown that abrading the epithelium of a cornea does not always lead to an infection, but if the stroma is damaged, even a small number of microbes can cause an infection (Lee, 2003). How then does an uninjured cornea allow bacteria to penetrate through the basal lamina? It is possible that the normal physiology of the basal lamina is altered due to subclinical inflammation caused by post-lens bacteria or other unknown causes.
The normal tear film has protective components that may become separated by the contact lens, therefore creating pre- and post-lens tear films. The post-lens tear film may not have good tear exchange, which may allow for the accumulation of inflammatory debris or microorganisms that would typically be removed via the tear film and blinking action. Dr. Fleiszig's current theory is that protective components of the tear film are not layered appropriately when a contact lens is on the eye, which therefore makes the eye more susceptible to infection (Fleiszig, 2010).
Another possible mechanism is the formation of biofilms on the contact lens surface (Behlau and Gilmore, 2008; Fleiszig and Evans, 2010). Biofilms are a mixture of bacteria held together by a secreted matrix termed extracellular polymeric substance (EPS) (Behlau and Gilmore, 2008). This matrix develops in steps and begins with planktonic (free floating) bacteria adhering to the surface of a material. The bacteria proceed to aggregate and begin to form small colonies. These colonies mature and are capable of communicating with each other (quorum sensing), which can enhance the organisms' ability to invade epithelial cells and increases the likelihood of compromising the basal lamina.
Biofilm formation can occur in less than one day, and even faster with hydrogel lenses (Stapleton et al, 1993; Szczotka-Flynn et al, 2009). Fleiszig and Evans (2010) have found that lenses contaminated with Pseudomonas and worn on an extended wear basis take almost one week to develop MK. When a biofilm-contaminated lens is placed on a naïve cornea, the infection occurs in two days (Tam et al, 2010). Therefore, the maturation of a biofilm most likely increases virulence and the risk of MK.
Szczotka-Flynn (2009) studied the effects of current contact lens solutions on biofilms and found that solutions containing biguanides were effective at reducing planktonic bacteria but had essentially no effectiveness against biofilms. Hydrogen peroxide solutions and polyquaternium-preserved solutions performed well against Pseudomonas and Staph aureus biofilms, with hydrogen peroxide solutions being superior for Serratia species (Szczotka-Flynn, 2009).
Diagnosis
While the mechanism of MK is not fully understood, there is clear progression in isolating a cause and it ultimately may result from a disruption in the tear film. All contact lenses allow for biofilm formation, but wearing lenses on an extended wear basis allows for increased contact time with the pathogens and cornea. Daily disposable lens wearers are not immune to MK, and it is possible that a tight-fitting lens may alter the protective mechanisms of tears, therefore making a cornea more prone to infection.
One of the primary differential diagnoses of a bacterial keratitis is an infiltrative keratitis, particularly a symptomatic one. Infiltrative keratitis can present as a contact lens peripheral infiltrate/ulcer, asceptic ulcer, or a marginal ulcer and may affect as many as 2 percent to 6 percent of patients in some way (Stapleton et al, 2007). As the names indicate, these conditions are more of an inflammatory response than an infectious process. The primary culprit is suspected to be exotoxins, or proteins secreted by bacteria. Individuals who overwear their lenses, top off solutions, wear lenses overnight, or have poor hygiene make themselves more susceptible (Stapleton et al, 2007).
Differentiating the two conditions may not always be straightforward. Typically MK lesions are greater than 1mm in size, create diffuse injection of the bulbar conjunctiva, cause an anterior chamber reaction with possible hypopyon, manifest as an excavated ulcer located centrally or paracentrally to the visual axis, and are very painful (Figures 1 through 3). Infiltrative ulcers tend to be smaller than 1mm, are usually located limbally or midperipherally, have more sectoral conjunctival injection, have an area of staining that is typically less than the area of the underlying infiltrate, and are usually not associated with an anterior chamber reaction (Karpecki, 2009) (Figure 4).
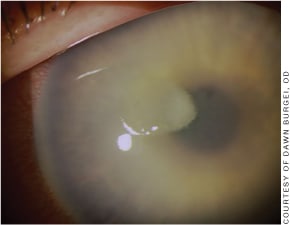
Figure 1. A Pseudomonas aeruginosa infection. Notice the large ulcerated lesion much greater than 1mm in diameter with surrounding edema as well as diffuse injection.

Figure 2. Paracentral ulcer with significant infiltration and edema.

Figure 3. Severe central ulcer with dense infiltration, edema, and hypopyon.
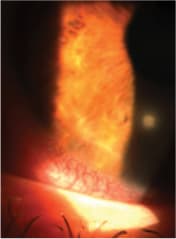
Figure 4. A contact lens peripheral ulcer with a diameter less than 1mm, sectoral conjunctival injection, underlying infiltrate, and surrounding corneal edema.
Organisms/Treatments
If you are confident that the lesion you are treating is inflammatory in nature, the use of a steroid/antibiotic combination will likely be successful. In fact, if the lesion is truly infiltrative, an antibiotic is essentially worthless, according to Melton and Thomas (2009). If there is any doubt as to whether or not the lesion is infectious, the use of an antibiotic is absolutely indicated as a steroid may hinder the immune response. It undoubtedly takes a few of these experiences to better identify the type of lesion in question.
One of the most common causes of contact lens-related MK continues to be Pseudomonas species (Bourcier et al, 2003; Mah-Sadorra et al, 2005; Keay et al, 2006; Kaye et al, 2010; Sueke et al, 2010). This species tends to be one of the most virulent organisms and therefore can be visually devastating, which may result from its ability to alter genes related to virulence, survival, and adaptation (Fleiszig, 2006). Other gram negative threats include Serratia spp. and Klebsiella spp. Infections secondary to gram negative organisms tend to be more costly and more severe compared to gram positive infections (Fleiszig, 2006; Keay et al, 2006).
Staphylococcus aureus and coagulase-negative Staphylococcus aureus tend to be the overall most common cause of bacterial keratitis (Constantinou et al, 2007; Kaye et al, 2010; Sueke et al, 2010). Fortunately these infections are typically not as severe as those caused by Pseudomonas, which are more frequent in contact lens-related MK (Cheng, 1999). Of recent concern, however, is the rise of methicillin-resistant Staphylococcus aureus (MRSA) (Rapuano, 2008). Infections with MRSA are typically difficult to treat, but are not typically associated with contact lens-related MK at this time.
Proper treatment of MK begins with proper diagnosis, and in many cases this requires a culture of the lesion. When to culture a lesion is up for debate; however, the American Academy of Ophthalmology recommends performing a culture for a non-responsive lesion, or if there is extensive infiltration into the stroma (Rapuano, 2008). Likewise, we advocate culturing any lesion larger than 1.0mm that is central or paracentral in location.
It is not possible to obtain instant analysis following a culture, so prompt treatment with a fourth-generation fluoroquinolone is a great start. Although gatifloxacin (Zymar, Allergan) and moxifloxacin (Vigamox, Alcon) do not have Food and Drug Administration (FDA) approval for bacterial keratitis, they have been shown to be just as effective as fortified tobramycin and cephazolin (Constantinou et al, 2007; Sueke et al, 2010). Previous-generation fluoro-quinolones ofloxacin, levofloxacin, and ciprofloxacin do have FDA approval for bacterial keratitis, but there has been evidence of some resistance to these medications (Wilhelmus et al, 2003). Regardless of the fluoroquinolone chosen to be used, it needs to be dosed approximately every 15 minutes for at least two hours, then every 30 minutes for at least two hours, and then hourly until the patient returns the next day for a follow-up visit. Some practitioners even recommend a topical ointment while the patient attempts to sleep (Rapuano, 2008). The use of a cycloplegic may help prevent a synechia and may make the patient somewhat more comfortable.
If the lesion is not improving with good compliance, it may become necessary to consult with or refer the patient to an anterior segment specialist, and fortified antibiotics will likely need to be implemented (Gangopadhyay et al, 2000). Typically these formulations are tobramycin/cephazolin or tobramycin/ vancomycin, with each formulation having both a gram positive and a gram negative component (Rapuano, 2008).
The use of steroids has been debated for years, and many practitioners believe that scarring may be reduced with their use. Steroids may decrease the body's immune response, which may help prevent the scarring; however, it could potentially intensify the infection. While there is no definitive evidence as to the clinical outcome, you should hold off on implementing steroids until the ulcerated lesion has re-epithelialized. A current study is underway to evaluate clinical outcomes and may settle the debate on the role of topical steroids (U.S. NIH − Steroids for corneal ulcer trial).
Prognosis
Approximately 13 to 28 percent of patients will have greater than two lines of vision loss following resolution of contact lens-related MK (Cheng et al, 1999; Keay et al, 2006; Stapleton et al, 2008). Typically the worse the initial presentation (i.e., a deep and/or large infiltrate, presence of corneal vessels, or an anterior chamber reaction), the worse visual outcome (Bourcier et al, 2003). Treatment delay is also related to poor outcomes as is the causative organism, with Pseudomonas usually the most common (Keay et al, 2006). Gram negative bacteria are often related to a worse visual outcome due to the higher virulence these organisms employ.
Conclusion
Contact lens wear increases an individual's risk of MK. MK with extended wear effects approximately 1 out of 500 people while use of any type of contact lens is associated with MK in approximately 1 out of 2,500 wearers. The risk of MK compared to other significant life risks is low (Szczotka-Flynn et al, 2009). Yet, with nearly 100 to 120 million contact lens wearers in the world, nearly 60,000 people may contract MK.
Further investigation of the eye's defense mechanisms as well as of the infectious mechanisms employed by microorganisms will hopefully lead to better preventive strategies. Improving our patient education on MK risks as well as properly educating them on contact lens hygiene may also help decrease the incidence of infection. We currently have very good medications available, and not many individuals who develop MK lose more than two lines of vision. Unfortunately, we do not have all the answers at this time. Possessing the tools to properly identify and treat contact lens-related MK is important because this condition will continue to affect people for the foreseeable future. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #177.