


ORTHOKERATOLOGY
An Update on Orthokeratology
New technology and lens designs are expanding the applications for orthokeratology treatment.
By Cary M. Herzberg, OD, FOAA

Dr. Herzberg has been practicing orthokeratology for more than 25 years. He is the founder, president, a board member, and a fellow of the Orthokeratology Academy of America. He is an advisory board member of the Gas Permeable Lens Institute, a contact lens design consultant to C&H Contact Lens, and he shares a patent for the first scleral orthokeratology design. |
This first decade of the new millennium could well be described as a decade of medical technological breakthroughs. Like the medical field in general, orthokeratology (or corneal reshaping) has seen its share of advances. Ten years ago many of us could not have anticipated all that would emerge as the modern practice of ortho-k progressed. Indeed, the process and tools that make up corneal reshaping today hardly resemble what I used in my ortho-k practice just a quarter of a century ago.
The purpose of this article is to present what constitutes a contemporary corneal reshaping practice as well as what may be in its future sights. Some of you may be surprised to learn how thoroughly ortho-k can meet the needs of a large percentage of your patient base.
It is not my purpose to endorse a particular ortho-k fitting style or lens design. It is also not feasible to cover all of the many different designs and their variations. In addition, please note that I will review many new areas of corneal reshaping practice in this article, some of which are not approved by the U.S. Food and Drug Administration. For example, utilizing corneal reshaping in correcting high myopia (>6.00D) would be considered an “off-label” use.
Safety and Efficacy
Practitioners and patients alike want the answer to one question in particular. How do we determine whether corneal reshaping is safe? Media coverage, clinical studies, and scientific papers can be a good place to initiate this process.
Reports have surfaced periodically in the media concerning incidents of microbial keratitis (MK) with ortho-k use. These reports primarily pertained to children in Asia and, unfortunately, some of these cases resulted in vision loss. A review of the literature failed to determine whether these children were actually fit by practitioners with ortho-k lenses. Questions were also raised pertaining to poor lens hygiene and lack of regulation of the modality (Jacobson, 2005). Furthermore, the preponderance of reported MK cases (69 percent) occurred around 2001, and a large segment of all of the reported cases (38 percent) were due to Acanthamoeba (Watt and Swarbrick, 2008).
A number of studies have been conducted that address the safety of orthokeratology including the Children's Overnight Orthokeratology Investigation (COOKI, Walline, 2008), Longitudinal Orthokeratology Research in Children (LORIC, Cho et al, 2005), Corneal Reshaping And Yearly Observation Of Nearsightedness (CRAYON, Walline, 2008), Stabilizing Myopia by Accelerating Reshaping Technique (SMART, Eiden et al, 2009), Overnight Corneal Reshaping (OCR, Lipson, 2009), and a study conducted at The Ohio State University (Bullimore, 2009). Each of these studies suggests that under controlled circumstances, ortho-k is safe. The results from the COOKI and CRAYON studies have concluded that 75 percent of children are capable of wearing corneal reshaping lenses. The SMART study is ongoing and will provide results for children ages 7 to 14 wearing ortho-k lenses for a five-year period.
The Ohio State study found that “the risk of MK with overnight reshaping lenses is similar to other overnight modalities” (Bullimore, 2009). The researchers obtained data from 86 randomly selected practitioners and 1,317 patients fitted during 2005 and 2006. The patients contributed 2,593 patient years of wear divided almost evenly between adults (49 percent) and children. Fifty event forms were submitted with 11 reporting corneal infiltrates. Two of these were MK, resulting in an estimated incidence of 7.7 per 10,000 years of wear. What does this all mean? That in all likelihood your corneal reshaping patients have a slightly higher risk of developing MK than your daily wear soft contact lens wearers do. Also, the risk of MK in ortho-k wearers may be as high as that for silicone hydrogel lenses worn overnight (Schein, 2005). Additional studies are needed to more completely address this issue.
When it comes to corneal reshaping safety, scientists commonly study corneal compromise during ortho-k lens wear. Does ortho-k compromise the epithelial barrier function and predispose the cornea to MK? Choo et al (2008) at the Institute for Eye Research set out to determine this by soaking ortho-k lenses in high concentrations of Pseudomonas aeruginosa and then placing them on cats' eyes for overnight wear. Pseudomonas aeruginosa is thought to be the leading causative organism (38 percent) in ortho-k infections worldwide (Watt and Swarbrick, 2008). The results of the study supported evidence that in cat eyes, ortho-k designs worn overnight do not compromise the epithelial barrier of the cornea.
Does the design of ortho-k lenses combined with overnight wear somehow make the lenses more susceptible to bacterial binding, which can lead to corneal compromise? Results so far from one study have shown that bacterial binding to ortho-k lenses had minimal short-term effects (Swarbrick, 2008).
The safety and efficacy of corneal reshaping will continue to be a hot topic in the years ahead. The many reports that have appeared in the media headlines have pertained primarily to “old” news and may reflect the lack of ortho-k knowledge and care in Asia 10 years ago rather than any unusual risks associated with corneal reshaping compared to other contact lens modalities.
Reports do continue to surface of MK incidence and corneal reshaping, requiring all of our due diligence. The eye health of your patients is your responsibility, making it mandatory that you seek to remain current in the practice of corneal reshaping. There are simple steps you can follow to maintain the health and safety of your ortho-k wearers' eyes. These include careful fitting of the ortho-k lenses, using a corneal topographer (essential in monitoring and troubleshooting), educating patients to not use tap water on their lenses and to replace lens cases monthly, patient compliance through education, and continuing with regular aftercare (Swarbrick, 2008).
What Happens to the Cornea During Ortho-k?
With the success of ortho-k, even for high myopes, questions arise regarding how such changes can be accomplished with movement of the corneal epithelium alone. Many studies have been conducted to attempt to explain the corneal changes that occur in ortho-k. A popular explanation for myopic refractive changes is that they result from movement of the corneal epithelium away from the center of the cornea and towards the periphery. With the corneal epithelial layer measuring approximately 50 microns, correcting myopia greater than 6.00D is mathematically not possible with epithelial thinning alone because an approximate 7 to 8 micron change in the epithelial depth accounts for approximately 1.00D of refractive change. So if the central epithelium alone were responsible for the refractive change, then correcting 7.00D of myopia with corneal reshaping would cause changes into the stroma (Berke, 2009).
Many theories have been presented to explain the changes in corneal tissue that result in the refractive changes in ortho-k. They attempt to explain corneal tissue changes as a result of epithelial cell compression, central thinning versus midperipheral thickening, midperipheral hyperplasia, increased cell retention, or decreased epithelial sloughing. So what exactly are we changing in the cornea itself that produces the ortho-k effect? Results from studies performed by Berke and colleagues may surprise you. Berke (2009) suggests that the central epithelial cells do not compress, thin, or migrate. “It appears as though the paracentral region thickens thus flattening the central cornea undergoing corneal reshaping. The induced minus lens sits on top of the pre-existing cornea, not embedded within it. The paracentral thickening appears to be essentially stromal hypertrophy rather than epithelial.” This new theory may well lead to many new lens designs including perhaps an optimum one. While this theory is a possibility, Cheah et al (2008) report that the changes are due to epithelial cell compression in the central cornea, so this issue needs to be further investigated.
Myopia Progression and Ortho-k
The National Eye Institute has just released new data on myopia which is sure to be of interest to even the most conservative practitioners. A current NIH study reported that in individuals aged 12 to 54, the frequency of myopia increased from 25 percent in 1972 to 41.6 percent in the five-year period studied (1999 to 2004). The study included people who had myopia ranging from mild to severe (Roan, 2009).
Reim and colleagues (2003) first reported the potential for myopia control with ortho-k lenses in a retrospective study reporting that patients corrected with corneal reshaping experienced about a 60-percent reduction in myopia progression. The LORIC study was conducted in Asia and reported a much slower rate of myopia progression and axial elongation (47 percent) among young progressive myopes who underwent corneal reshaping compared to those who wore eyeglasses. The CRAYON study also found lower rates of myopia progression and axial elongation (57 percent). Both the LORIC and CRAYON studies were small in scale, involving fewer then 40 subjects. The SMART study, a large-scale (300 subject), five-year, longitudinal multicenter evaluation of the effectiveness of corneal reshaping for young progressive myopes, is now underway.
Image Shells and Ortho-k: Preventive Care With the discovery of the phenomenon of form deprivation myopia, research has demonstrated that ocular growth and refractive development are regulated by visual feedback associated with the eye's refractive status. The conclusions of Dr. Earl Smith and colleagues (2009) point to the peripheral retina in primates as being more influential for controlling eye growth than previously thought possible. When susceptible visual systems are corrected with myopic lenses, it creates an image shell described as a positive curvature of field. These visual systems, while being corrected centrally, suffer from a relative hyperopia peripherally that causes conflicting visual stimulus. The result is elongation of the eye to correct the peripheral hyperopia. If, however, the peripheral retina is experiencing a relative myopia effect (negative curvature of field), then elongation may slow. The measurement of this discrepancy between peripheral and central retina is performed via peripheral refraction (Mutti, 2007).
Unlike conventional methods of correcting myopia such as glasses or regular contact lenses, myopia-correcting corneal reshaping lenses create a negative image shell on the retina of a treated patient (Figure 1). It is not yet apparent what ortho-k design is optimal to accomplish the best image shell. It may also be possible to track changes in peripheral refraction through corneal topography. Future research will include the optimization of orthokeratology to correct peripheral refractive error and the development of testing equipment that can measure a patient's susceptibility to develop myopia based on peripheral refraction (Mutti, 2007). This could lead to early treatment with corneal reshaping of those patients most susceptible to axial elongation of the eye (Cross, 2008). It is with great optimism that I look forward to a future of improved, efficient, and efficacious delivery of corneal reshaping products to solve our patients' corneal and refractive conditions.
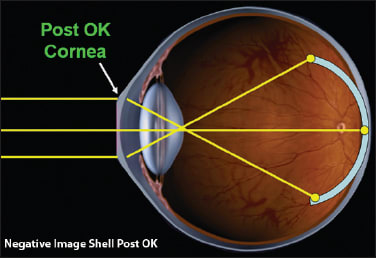
Figure 1. Negative image shell post-orthokeratology treatment.
Getting Started With Ortho-k
The FDA has approved ortho-k for the treatment of up to 6.00D of myopia correction. With the advancement in computer driven lathing systems that have a tolerance of 0.0001mm, incredible accuracy is now available. With the advent of no polish blends, this accuracy and repeatability have risen to levels never before seen. This has allowed for advanced computer programs with data collected over thousands of fits to design for best results.
Today, even a novice ortho-k practitioner can attain success rates that were previously achieved only by contact lens design experts. Supplying keratometry values, manifest refraction, horizontal visible iris diameter (HVID), and, in some cases, corneal eccentricity values are all that is needed to successfully fit a low-to-moderate myope. Early results from the SMART study using the Euclid Emerald ortho-k lens indicated a first-fit success rate of 80.5 percent. In addition, the researchers reported a 95-percent success rate with only one additional lens fit. Very effective empirically fit designs are available throughout the industry that require only keratometry values, manifest refraction, and HVID values including lenses from Bausch + Lomb's Vision Shaping Treatment (Contex, DreamLens, Euclid, Wave), Paragon Vision Sciences (Paragon CRT), and Global OK (GOV).
If at first you don't succeed, laboratories have extremely competent consultants to answer questions and troubleshoot any problems that you may have. But sometimes even they need the ‘expert.’ As an example, TruForm Optics will ask Dr. Tom Reim, who designed the DreamLens, to consult with them on challenging cases.
Practitioners can now use the SureFit (Paragon) dispensing system to provide increased initial fitting success rates by utilizing a multiple (three) diagnostic lens pack. The lenses are chosen based on data from thousands of successful lens fit outcomes. This system can help reduce chair time and patient adaptation during the initial wearing schedule. Diagnostic sets can also offer added convenience and instant gratification with a greater range and availability of lens parameters. You can order small, medium, or large sets ranging from 10 to more than 100 lenses designed either by the laboratory or by you. With powerful computer-driven programs such as OrthoTools (www.orthotools.com), an optimum fitting set may be designed based on a number of factors including corneal eccentricity and optimum tear film thickness. The data can be integrated with diagnostic lens fitting to achieve a best fit lens design.
Using Topography Software to Design Ortho-k Lenses
Paralleling the meteoric rise in lathing technology have been advancements in topographical analysis of the cornea. Modern topographers have reached a level of acceptable accuracy and repeatability. The limitations on acquiring good topography images have more to do with the operator maintaining focus and alignment during their acquisition.
While topographer designs have improved in this regard, the greatest advances have come from topography software (Dave, 2008). Powerful computer programs can now analyze topographical maps to design corneal reshaping lenses. This computer design process can also involve a small fitting set of lenses to facilitate the outcome.
The topography-based software from BE Vision Shaping Treatment (B+L) chooses the first lens, and patients return after wearing the lenses overnight to determine how close the “bulls-eye” pattern is to optimum. The best bulls-eye results may come from the initial trial lens or from a new lens selected by the program from the fitting set. Another popular program from Wave Contact Lenses is a CAD/CAM system that integrates several features working together for optimum outcomes. Along with corneal topography, one program is used to manipulate design features, then another software program is used to send the design features as a numerical file to a CNC lathe. This allows you to custom design a patient's ortho-k lens to meet the data supplied through the topography in a precise and accurate manner.
High Myopia No Longer Out of Reach
Progressive myopia is on the rise and is causing a greater incidence of severe myopia. With this demand have come new corneal reshaping designs and philosophies including five-curve lenses, double reverse curves and dual geometric (DG) designs (Figure 2). Performing corneal reshaping safely and effectively beyond 5.00D of myopia with good all-day vision requires more manipulation of the corneal surface. That may mean a design that not only induces central flattening but also creates midperipheral thickening to sustain the visual outcome.
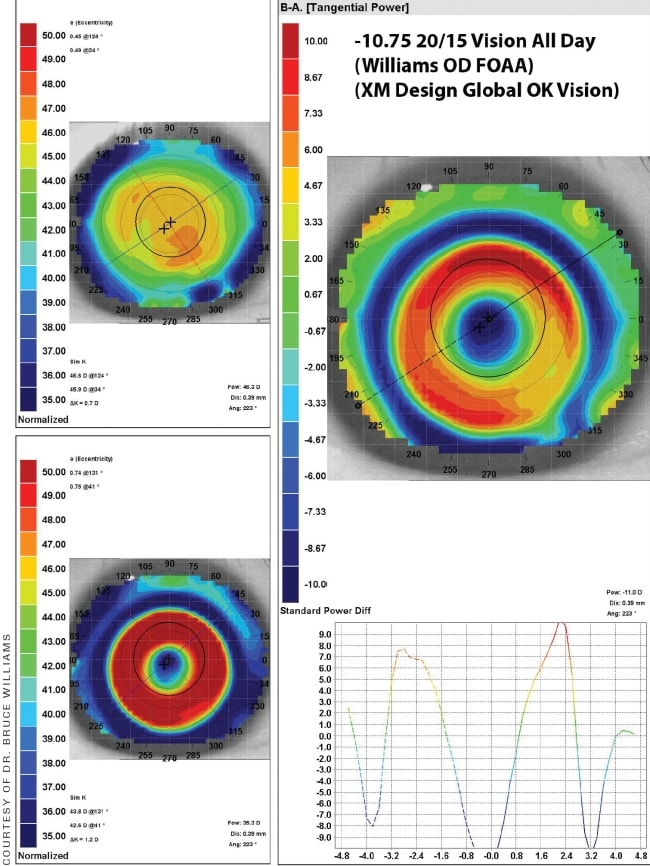
Figure 2. Bulls-eye corneal topography of a −10.75D myopic patient who achieved 20/15 unaided vision with orthokeratology.
In addition to enhanced lens designs, high myopes may also require additional lens fittings during the treatment phase for optimum results. It should be emphasized that corneal reshaping on prescriptions beyond 6.00D will result in much smaller treatment zones (Munnerlyn's Formula). This may result in night vision problems. Inform your patients of any possible complications that may result from corneal reshaping before you begin treatment. This should include any night vision problems that may result from glare or flare due to small treatment zones.
Presbyopic Corneal Molding
Corneal reshaping specialists have a secret weapon when it comes to correcting presbyopia. Due to a pinhole effect created by the corneal reshaping process, wearers who are early-to-moderate presbyopes can often still see adequately during close work. In the past, to supplement this effect, orthokeratologists could under-correct the non-dominant eye and create a monovision effect. Today, progressive molding designs offer more options.
One design was born from past experiences of fitting lenses too flat and creating superior decentration. This positioning, combined with central flattening, would create an inferior steep crescent or ‘smiley face.’ Patients gazing down through the steepened zone would experience a bifocal effect. To utilize this concept without the need for lens decentration, an additional aspheric zone was added to a traditional myopic design. This procedure flattens the central cornea for improved distance vision, but it also steepens the paracentral cornea, thereby creating a built-in bifocal or multifocal zone right on the cornea (Figure 3).
COURTESY OF PATRICK J. CAROLINE, FAAO
Figure 3. OK Multifocal (Contex).
Another design offers options such as a central reading button with a relatively flat outer ‘plateau’ zone that reshapes the cornea into an annular zone for distance vision. This design (Global OK) centers well due to an aspheric alignment zone. These designs have brought a whole new area of focus to corneal reshaping practice.
Correcting Astigmatism With Ortho-k
The model of forces acting in ortho-k makes it difficult to fully correct high levels of “bowtie” with-the-rule astigmatism. In fact, limbus-to-limbus astigmatism has been one of the few contraindications to ortho-k treatment (Mountford, 2004).
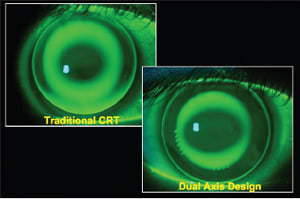
But how times have changed! New lathe technologies and powerful computer programs make it possible to customize lenses like never before. Need a toric alignment curve or an oval pupil in response to corneal astigmatism? Many designs now offer these options and more to solve challenging astigmatism fits. Going further, we now have available the Paragon CRT Dual Axis design (Paragon), a later-generation lens based on the original design that maintains its profile with the return zone depth (RZD) and landing zone angle (LZA) over 360 degrees. The Dual Axis, while not a true toric design, has two separate RZDs and perhaps two different LZAs 90 degrees apart (Figures 4 and 5).
COURTESY OF PATRICK J. CAROLINE, FAAO
Figure 4. Fluorescein pattern of a standard spherical Paragon CRT lens and of a Paragon CRT Dual Axis lens on a toric cornea.
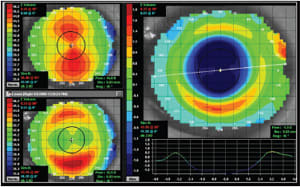
Figure 5. Dual Axis design patient topography.
Ortho-k for Hyperopia
Some of the most effective early designs for ortho-k correction were products of aspheric technology. Posterior-aspheric designs of 0.8 eccentricity or greater commonly found in rigid lenses designed for correcting presbyopia generated significant reading adds, particularly on steep corneas. A negative side effect of such designs was central corneal steepening, which caused a myopic shift in the prescription.
This is the case with hyperopic ortho-k. A steeper central cornea is created by gently and precisely squeezing the midperipheral cornea. These designs are 100 percent aspheric while providing adequate tear exchange. They tend to work more slowly when compared to myopic ortho-k. A good lens fit must exhibit central clearance over the optical zone and progress to midperipheral touch while maintaining adequate edge lift. Like all ortho-k lenses, such a design must center well.
Another alternative is to adapt a Paragon CRT design. Lens selection is similar as that for myopic correction, but the sagittal depth of the RZD is reduced by 50 microns while maintaining the same landing angle. The base curve radius and power are adjusted to create the desired steepness in the central cornea.
Several designs or systems are available that can effectively correct up to 3.00D of hyperopia (Figures 6 to 8). It is now possible to even design a hyperopic progressive molding lens. How about a dual geometric bifocal design? The Global OK lens features a steep-flat-steep-flat design from the center to the periphery. It has central steepening for distance vision and a relatively flat outer plateau second zone. Aspheric curves can fine-tune the fit.
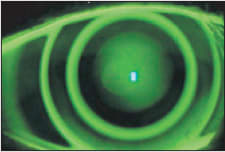
Figure 6. Dual Geometric Design (Global OK).

COURTESY OF PATRICK J. CAROLINE, FAAO
Figure 7. Hyperopic Multifocal Design (Contex).
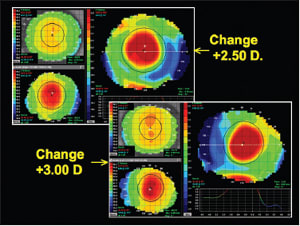
Figure 8. Corneal topography of hyperopic molding.
Corneal Rehabilitation Post-LASIK and for Keratoconus
With the increasing popularity of Laser-Assisted In Situ Keratomileusis (LASIK) vision correction, the number of potential patients needing solutions to less-than-optimal outcomes is likewise increasing exponentially. This need has created specialty practices in corneal rehabilitation of post-surgical corneas. Ortho-k fitting of such corneas is a natural extension of these practices (Williams, 2006) (Figure 9). In fact, ortho-k fitting is preferable to enhancements in part because these corneas are already thinner as a result of the original LASIK surgery. The added incentive for these patients is the freedom from wearing correction during waking hours that ortho-k can provide, especially after they have already made a significant investment to gain freedom from contact lenses or glasses.
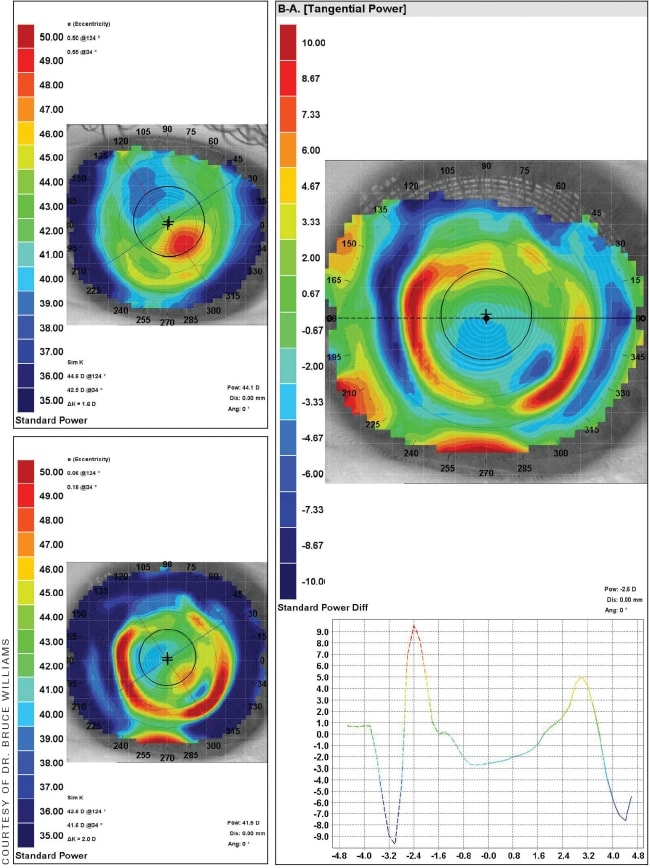
Figure 9. Topography of post-PK ectasia treated with Paragon CRT.
Typically a conventional ortho-k design is successful, but modifications such as increased treatment zone sizes can be beneficial for night vision issues. As with most ortho-k fits, one of the key factors is selecting the appropriate overall lens diameter. Because of the oblate surface that is being treated, the best results will occur when the overall lens diameter covers about 90 percent of the cornea. If you have the pre-surgical keratometry readings and manifest refraction, you can select the best-fitting lens as if the patient had never undergone LASIK. If those findings are not available, diagnostic lenses will usually resolve any questions.
Not long ago, keratoconus was on the list of absolute contraindications for corneal reshaping (Mountford, 2004). Today, fascinating results are being attained in correcting mild-to-moderate keratoconus with ortho-k (Yamada et al, 2005). A study sponsored by Hadassah Medical Organization is exploring the safety and efficacy of treating moderate keratoconus with ortho-k lenses (Landau, 2008).
Keratoconus has its own set of unique characteristics when it comes to corneal molding. The exact apical curvature of the cone and how far it's decentered from the geometric center of the eye are very important. Another challenge is to determine the best alignment curve for the ortho-k lens, which can typically be performed using accurate corneal topography. If the moderate cone has caused extensive corneal distortion, diagnostic fitting for the best alignment curve may be necessary. As in post-LASIK rehabilitation, it is important to have the optimum overall diameter, for which an accurate measurement of HVID is required. Determine the final base curve radius and power through diagnostic fitting. Often your most valuable tools in fitting keratoconus with ortho-k is accurate corneal topography and an ortho-k diagnostic set (Figure 10).
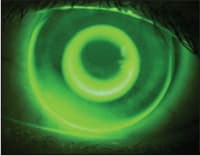
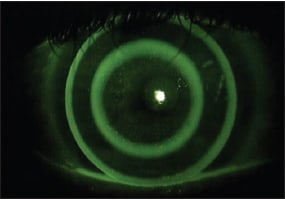
Figure 10. Bulls-eye fluorescein pattern in keratoconus (Global OK design).
A Tale of Two Countries: A Global View
China and the Netherlands appear, in general, to have little in common. When it comes to ortho-k, however, the world's most populous country may have taken some lessons from one of the smallest. The Netherlands model is a working success story for corneal reshaping. It certainly helps that the Netherlands is home to a number of ortho-k innovations and that practitioners from there have a history of fitting a high percentage of their patients with GP lenses. Ortho-k had its roots in the United States, but came to the European continent and to the Netherlands in 2003. In the Netherlands, right from the start the perception was that ortho-k fitters needed training and that no practitioner should fit these lenses without a corneal topographer (Beerten, 2004). In fact, the systems that came forth (NKL, Procornea) were topography-based. A fitter would submit refractive and corneal topography data from which lenses were designed.
The most likely candidate for ortho-k in the Netherlands is a young adult, and 6 percent of all contact lenses fit in the Netherlands are for ortho-k (van der Worp, 2008).
China, conversely, had a slightly different experience. China's ortho-k community is a small but dedicated group of researchers, educators, and practitioners who—until recently—were based mostly in Hong Kong. China banned ortho-k after citing the dangers posed to the population from an unregulated and unsupervised industry. This ban lasted until 2007 when the Chinese government approved an ortho-k design for overnight wear.
These were some hard lessons for the most populous country in the world. The lack of regulation and training was a disaster for all concerned. More recently, steps have been taken to emphasize education, training, and tighter regulation with regard to ortho-k.
With more than a 70-percent frequency of myopia among elementary age children in China, the driving force behind ortho-k implementation is myopia control (Fan, 2004). Also impacting ortho-k is a change in demographics in China over the last 10 years. Unlike a decade ago when there were almost no private hospitals or clinics, today they play a much more important role in the healthcare delivery system.
New Ortho-k Applications
New areas of research in myopic ortho-k involve semi-scleral ortho-k designs and the use of soft contact lenses for corneal reshaping (Caroline, 2008). I presented a paper at the 2004 Global Orthokeratology Symposium on using corneal-scleral lenses with ortho-k (Herzberg, 2004) (Figure 11). I still have well over 100 patients wearing the lenses successfully. At the time I used the Macrolens (C&H Contact Lens) mini-scleral design, which ranges in overall diameter from 13.6mm to 15.3mm. Mini-scleral lens designs are a very safe and useful medium for ortho-k correction, and they almost always create a well-centered treatment zone.
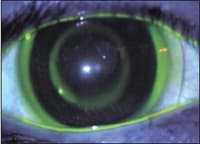
Figure 11. Corneal-scleral lens design.
The discovery of improved vision in high myopes who had mistakenly worn Night & Day (Ciba Vision) silicone hydrogel lenses everted for extended periods of time has led to new research in this area. The flexure of these materials appears to be optimum for reshaping the cornea. Currently, the total maximum correction is about 2.00D with new designs on the way (Caroline, 2009). This may offer an alternative for low myopes who have a problem with the initial lens awareness of rigid corneal reshaping lens designs.
Future Applications: Crosslinking
When we look back at the first decade of our millennium, we may conclude that it was the time when the promise of genetic engineering and smart drug delivery systems started becoming a reality. Although not quite as much of a paradigm shift, orthokeratology has its own great story to tell. With corneal crosslinking we are on the doorstep of a great new era in corneal reshaping. Crosslinking is a process that improves corneal rigidity by increasing the chemical bonds between the collagen fibers. It is a physiological procedure that causes the corneal stroma to become less flexible, thus making it stiffer by increasing the biomechanical strength of its tissue structure. It shows great promise in reducing the need for enhancement procedures following LASIK. It can control the progression of ectasia in keratoconus. It can prolong the correction achieved by corneal molding.
One way to crosslink the cornea is to add a photo-reactive reagent to the stroma and “cure” it with ultraviolet A light. Early results have concluded that the procedure is safe, with some patients showing a reduced dependence on wearing corneal reshaping lenses (El Hage, 2009). Another way is to use decorin (Stableyz, Euclid Systems) as a natural cross-linking molecule. Preliminary results are very encouraging with several patients not having to wear their moldings after the initial treatment for up to a year. The product will be taken to the FDA with a request to initiate clinical trials in the United States in 2010.
Sharing an Exciting Future
Today's eyecare practices face many challenges as they strive to grow into the new decade. The economic downturn is causing many of our patients to delay eyecare decisions or to seek cost cutting alternatives to eyecare services and products.
Corneal reshaping is an area that offers an incredible growth opportunity for practice. With a well thought out internal marketing program accompanied by staff and practitioner training, a practice can reasonably and quickly “turn on” their existing patient base to corneal reshaping.
The Orthokeratology Academy of America's (www.okglobal.org) annual education meeting will take place Oct. 20 to 24, 2010 near Chicago and offers a comprehensive program for practitioners and staff entirely on corneal reshaping. Included in the program is an all-day “boot-camp” for first-time or inexperienced ortho-k fitters.
With the emergence of the ortho-k specialty and all of the ways you can utilize its many applications, you have many new and innovative answers to the challenging marketplace we all live in. The question is, will you take the time to educate your patients about the benefits of corneal reshaping or potentially lose out on its exciting future because they hear about it somewhere else? The choice is yours. CLS
I would like to thank Dr. Bruce Williams (Seattle, WA), Jonathan Jacobson (Menicon), Marcel Kopito (Bausch + Lomb), Steven Ernst (Contex), Dr. Tung Hsiao-Ching (Global OK), PM Hawkins (Paragon Vision Sciences), Dr. Bruce H. DeWoolfson (Euclid Systems), Dr. Mark Bullimore (The Ohio State University), and Joann Simonsen (Euclid Systems) for taking time away from their busy schedules to provide information and support for this article.
For references, please visit www.clspectrum.com/references.asp and click on document #172.