


contact lens case reports
Contact Lenses Following Corneal Trauma
BY PATRICK J. CAROLINE, FAAO, & MARK P. ANDRÉ, FAAO
The irregular astigmatism and frequent anisometropia that develops after corneal trauma is often best corrected with some form of contact lens. Corneal trauma results in some rather predictable topographical changes. However, these depend on many factors including injury location, patient age at time of injury, and healing (spontaneous or with surgical intervention).
From a contact lens fitting perspective, perhaps the two most important topographical caveats are: the cornea flattens over any laceration; and the corneal flattening effects increase as the laceration approaches the visual axis.
GP Fitting Post-Corneal Trauma
Our patient is a 34-year-old male who suffered a plastic foreign body injury to his left eye that remarkably never penetrated the iris or the crystalline lens. The corneal topography of the traumatized eye showed topographical flattening over the laceration site (Figure 1). The topographical flattening increased as the wound approached the visual axis.
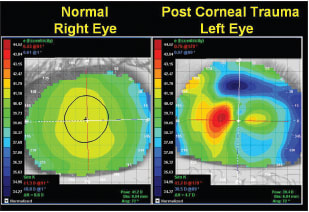
Figure 1. Corneal topography of the normal right eye and that of the traumatized left eye.
In cases in which a wide range of asymmetrical curvatures are present throughout the cornea, we select the base curve of the initial diagnostic lens by a technique we call “mean topographic curvature.” In this technique we use the normalized scale of the axial map to identify topographical endpoints of the given cornea, with the steepest portion of the cornea represented in red and the flattest in blue. The remaining 14 colors identify the curvatures that make up the rest of the cornea.
Because there are a total of 16 colors that represent the range of corneal curvatures, we simply count up eight colors (boxes) from the bottom and select a lens with a base curve radius equal to the mean topographic curvature (Figure 2). In this case it was 39.00D or 8.65mm.
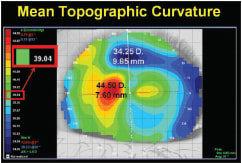
Figure 2. Initial base curve radius selection with the mean topographic curvature technique.
We selected the 39.00D (8.65mm) base curve, 10.8mm lens from our Clearion, Dual-Hinge (Acuity One) diagnostic set and applied it to the patient's eye. Note in Figure 3 the fluorescein pattern of this lens shows approximately 0.50D to 1.00D too much touch. However, it is clear that the mean topographic technique served us well in selecting the initial lens to evaluate.
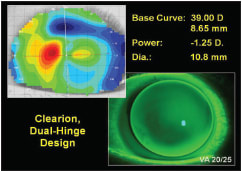
Figure 3. The fluorescein pattern of the initial diagnostic lens.
We performed a manifest refraction over the −3.00D diagnostic lens, resulting in a best-corrected VA of 20/25. The final lens had a 39.50D base curve, −1.25D, 10.8mm diameter. CLS
Patrick Caroline is an associate professor of optometry at Pacific University. He is also a consultant to Paragon Vision Sciences. Mark André is an associate professor of optometry at Pacific University. He is also a consultant for CooperVision.