


CL COMPLICATIONS
Diagnosing and Managing Lens-Related Complications
Correct diagnosis and effective management will help you return patients to healthy contact lens wear.
By Gregory W. DeNaeyer, OD, FAAO

Dr. DeNaeyer is the clinical director for Arena Eye Surgeons in Columbus, Ohio. His primary interests include specialty contact lenses. He is also a consultant or advisor to MedLens Innovations, Inc. Contact him at gdenaeyer@arenaeyesurgeons.com. |
The contact lens industry has made significant strides toward improving contact lens materials, designs, and solutions in the last 30 years. This has resulted in a higher percentage of patients who are able to comfortably wear lenses that provide them with glasses-free vision.
But complications can arise, even in patients who are carefully fit, educated, and compliant. Complications can be minor and may result in discontinuation of lens wear only if they affect vision or comfort, but they also may be sight-threatening. This article will review seven common contact lens complications and how to diagnose and manage them to get affected patients back to healthy lens wear.
Solution Reactions
A typical contact lens patient is potentially exposed to numerous active ingredients and preservatives contained in contact lens cleaning and soaking solutions, artificial tears, ophthalmic medications, and saline solutions. Exposure to these substances can lead to an allergic or toxic response to a particular product.
Patients who develop hypersensitivities to contact lens solutions will have symptoms that can include discomfort during lens wear, redness, and itching. Slit lamp findings may show one or more of the following: diffuse bulbar conjunctival injection, significant lower lid follicular reaction, superficial punctate keratitis (Figure 1), and/or lid dermatitis.
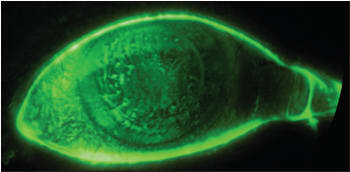
Figure 1. Severe superficial punctate keratitis secondary to hypersensitivity to contact lens solution.
A diagnostic dilemma is that these signs and symptoms may mimic or can overlap signs and symptoms of seasonal or perennial ocular allergies and/or dry eye. Furthermore, if the hypersensitivity is a delayed type IV response, then it can take months of exposure to a particular antigen before a patient becomes symptomatic. For example, you may not initially suspect that a patient's symptoms stem from a problem with a multipurpose solution if the patient has successfully used that solution for months or years. Once a patient is sensitized to a particular antigen, any exposure will cause an immediate response. So a typical contact lens patient who has previously been asymptomatic and develops a hypersensitivity will suddenly manifest a bilateral allergic type response with contact lens wear.
The first step to manage this complication is to have patients discontinue contact lens wear and any current ophthalmic drops or solutions. Instruct patients to use non-preserved artificial tears until they are symptom free. If you suspect that a patient's care system is the antigenic source, then switch solutions, preferably to a hydrogen peroxide system to avoid other hypersensitivities. Refitting the patient to a daily disposable lens is another good option.
Contact lens-associated solution problems manifest as diffuse superficial punctate keratitis. This has been associated with specific lens and lens solution combinations (Andrasko and Ryen, 2008). Although usually asymptomatic, there has been a reported association between corneal staining and corneal infiltrative events (CIEs), and those who have high levels of staining may experience discomfort (Carnt et al, 2007; Andrasko and Ryen, 2008).
The key to managing these patients is making the correct diagnosis. Solution toxicity should be in the differential of any patient who presents with bilateral diffuse superficial punctate keratitis, which can sometime be accompanied by infiltrative keratitis (IK). Managing this complication involves instructing patients to discontinue lens wear and use artificial tears as a palliative treatment until they are symptom free. Use a different care system when reintroducing such patients to contact lens wear. Hydrogen peroxide has the lowest frequency of solution-induced corneal staining and CIEs with silicone hydrogel lenses (Carnt et al, 2009).
Superior Epithelial Arcuate Lesions
A superior epithelial arcuate lesion (SEAL) is a soft contact lens phenomenon that may cause affected contact lens patients to complain of irritation or foreign body sensation. The typical presentation is an arcuate area of corneal staining that can run from the 10 o'clock to the 2 o'clock position within 1mm of the limbus. After lens removal, this area will stain with fluorescein. Although not completely understood, the erosive area is probably the result of mechanical friction of the lens on the cornea. The highest frequency of SEALs seems to come from patients who wear high-modulus silicone hydrogel contact lenses, although design and diameter also most likely play a role in SEAL development (Carnt et al, 2009). It has been suggested that a lens that vaults excessively across the superior cornea can result in the upper lid collapsing the lens against the cornea, causing the friction necessary to produce epithelial defects (Caroline and André, 2009). The lesions rarely involve infiltrates or scarring.
Management involves discontinuation of lens wear and lubrication with artificial tears until resolution. To avoid recurrence, refit patients into a contact lens with a lower modulus or different design.
Contact Lens-Induced Papillary Conjunctivitis
Contact lens-induced papillary conjunctivitis (CLPC) is a more specific term that describes giant papillary conjunctivitis (GPC) that results from contact lens wear. Although its pathogenesis is not completely understood, it is classified as a type I and type IV immunologic response to coated and deposited contact lenses (Katelaris, 1999; Stapleton et al, 2003). Additionally, mechanical irritation from deposits or high-modulus soft lens materials may cause the release of inflammatory mediators that contribute to CLPC (Ballow et al, 1989; Ehlers et al, 1990). Patient symptoms include decreased lens tolerance, increased lens awareness, excessive lens movement, increased mucus production, redness, burning, and itching (Donshik et al, 2008). Giant, hyperemic papules (Figure 2), which may be generalized or local, will be evident on the upper tarsal plate (Skotnitsky et al, 2006). Patients who have generalized CLPC have more frequency of symptoms, and localized CLPC is more likely to result from silicone hydrogel lens use.

Figure 2. Contact lens papillary conjunctivitis.
The critical step to diagnose CLPC is to flip patients' lids. Any contact lens patient who complains of irritation with contact lens wears needs to have his lids everted to rule out or diagnose CLPC. Replacement frequency of soft contact lenses appears to be a primary factor in the development of CLPC. A retrospective study by Donshik and Porazinski (2000) of 47 newly fit soft contact lens patients showed that the incidence of CLPC was 36 percent in patients who replaced their lenses at four weeks or longer, but only 4.5 percent in patients who replaced their lenses at less than four weeks. No patients who were wearing two-week replacement or daily disposable contact lenses developed CLPC.
Returning patients who have CLPC to comfortable lens wear seems dependent on temporary discontinuation of lens wear followed by prescribing a more frequent replacement lens modality. Another study by Donshik (1994) of 221 patients who had CLPC showed that when contact lens use was not discontinued, only 50 percent of patients could continue wearing their lenses if their cleaning regimen was changed while 78 percent could continue lens wear if they replaced their lenses. However, in the same study, patients who discontinued wearing their lenses for three to four weeks had success rates of 68 percent for patients who resumed wearing their previous lens, 81 percent if they were refit with a GP, and 91 percent if they were refit into a frequent replacement lens modality.
Manage CLPC by having patients discontinue lens wear for three to four weeks and then fitting them into a more frequently replaced lens modality with a preference toward daily disposables. Consider prescribing a mast cell stabilizer/antihistamine to help speed recovery in those patients who have more severe responses. The upper tarsal inflammation will resolve as the CLPC improves, but it may take significant time for the papules to reduce in size and diameter, and the tarsal conjunctiva may remain thickened (Donshik et al, 2008).
Corneal Infiltrative Events
Infiltrative Keratitis is an inflammatory event for soft contact lens patients. Affected patients may be asymptomatic or have mild to moderate pain, and depending on the etiology it may be in one or both eyes. Affected eyes will have multiple small (<1mm) infiltrates of the anterior stroma, without an overlying epithelial defect, in the midperiphery to periphery with some diffuse infiltration (Sweeney et al, 2003) (Figure 3). The conjunctiva will be diffusely injected. IK may be associated with contact lens solution-associated corneal staining, tight fitting lenses, and Staphylococcal hypersensitivity, as the lens may harbor gram positive organisms (Szczotka-Flynn, 2009).
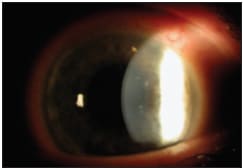
Figure 3. Multiple midperipheral infiltrates in a case of infiltrative keratitis.
Resolution depends on eliminating the trigger source. Because IK is non-infectious, treatment with antimicrobial agents is unnecessary. Have patients discontinue lens wear until they are back to baseline. If you suspect a hypersensitivity/toxicity issue, try switching to a peroxide care system or refit daily disposables. Lid hygiene and daily disposable lenses may help with Staphylococcal hypersensitivity, or refit looser lenses if their previous contact lenses exhibited late-day tightness.
Contact Lens-Induced Acute Red Eye (CLARE) is a sterile inflammatory event of the cornea and conjunctiva that is similar to IK except by definition it occurs upon awakening during extended soft contact lens wear. Symptoms include irritation, moderate pain, and photophobia. The cornea will generally develop small (<1mm) anterior stromal infiltrates in the midperipheral to peripheral cornea. These infiltrative polymorphic neutrophils (PMNs) are thought to be induced by a hypersensitivity reaction to exotoxins and endotoxins from gram negative bacteria, and this situation is exacerbated by the pro-inflammatory state of the closed eye during lens wear (Sankaridurg et al, 1996; Holden et al, 1996).
Because CLARE is a non-infectious event, management consists of lens discontinuation and palliative treatment until signs and symptoms resolve. Patients may then resume lens wear, but on a daily wear schedule.
Contact Lens Peripheral Ulcer (CLPU) A CLPU is a CIE that is more common in patients who wear lenses on an extended or continuous wear schedule (Stapleton and Wilcox, 2003). CLPU manifests as a peripheral focal infiltrate of PMNs less than 2mm in size that is well circumscribed (Figure 4) with diffuse infiltration and an overlying epithelial defect (Sweeney et al, 2003). Bulbar injection is usually confined to the quadrant adjacent to the infiltrate (Aasuri et al, 2003). Animal models have shown that this type of CIE can occur in the presence of S. aureus and a break in the corneal epithelium, which allows for access to bacterial exotoxins. Thus, CLPU is more likely to occur if a patient's contact lens harbors bacterial colonies or biofilms and is causing epithelial disruption.

Figure 4. A peripheral focal infiltrate in CLPU secondary to continuous wear.
CLPU is a non-sight-threatening, self-limiting event that will resolve with the discontinuation of contact lens wear, although a scar will form at the site of the focal infiltrate. Topical ophthalmic treatment is rarely needed, as symptoms will improve relatively quickly upon lens removal. CIEs such as CLPU do not appear to be a marker for increased risk of microbial keratitis (MK) (Sweeney and Naduvilath, 2007). However, as will be discussed next, the signs and symptoms of CLPU can overlap those of MK. When in doubt, especially if you cannot closely monitor a patient, a conservative approach is to start the patient on monotherapy of a fluoroquinolone.
Microbial Keratitis
MK remains the most serious complication of wearing contact lenses, and advances in the development of silicone hydrogels and daily disposables lenses have not reduced the incidence of this potentially sight-threatening event (Stapleton et al, 2008). Most contact lens-related MK is secondary to bacteria, with Pseudomonas involving more than half of these cases (Keay et al, 2006). For an infection of the cornea to occur, the offending organism must bind to and penetrate the corneal epithelium. Contact lens-induced hypoxia can cause compromised corneal epithelial integrity, impaired wound healing, and increased bacterial binding, which may predispose a patient to infection (Madigan and Holden, 1992; Mauger and Hill, 1992).
Patients who have MK will experience moderate to severe pain, photophobia, redness, and discharge. Slit lamp findings will show a focal, irregular stromal infiltrate greater than 1mm in size that may occur in the central, midperipheral, or peripheral cornea along with diffuse infiltration and an overlying epithelial defect (Aasuri et al, 2003) (Figure 5). Other findings include lid edema, diffuse general and limbal conjunctival injection, anterior chamber reaction, and possible hypopyon. As discussed earlier, the signs and symptoms of an early MK case can overlap with a severe CLPU. However, unlike CLPU, lens discontinuation will not result in improvement; in fact, without proper antimicrobial treatment patients will rapidly get worse. The take-home message is to treat any suspicious CLPU as MK until proven otherwise, as a delay in treating MK can significantly worsen prognosis.
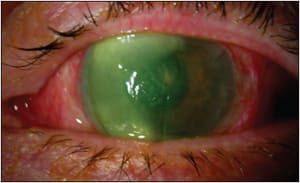
Figure 5. Severe bacterial microbial keratitis.
The effectiveness of fluoroquinolones has significantly changed the way that MK is managed. For one, not all cases of MK are cultured at the time of diagnosis. However, consider culturing the following cases: a centrally located lesion, a lesion that is >2mm, one in which empirical fluoroquinolone therapy has failed, and any monocular or immunocompromised patient (Edwards et al, 2004). If your office is not equipped to culture, then this would an appropriate time to refer patients to a corneal specialist.
Regardless of culturing, you should immediately treat suspected cases of MK with a fluoroquinolone. Remember, fluoroquinolones are concentration dependent, so start patients on an initial dosing frequency of every 15 minutes. The standard of care is to use one of the newer-generation fluoroquinolones, which include gatifloxacin (Zymar, Allergan), moxifloxacin (Vigamox, Alcon), and levofloxacin (1.5%, Iquix, Vistakon Pharmaceuticals). These fluoroquinolones have a broad spectrum of coverage for both gram positive and gram negative bacteria by interfering with the bacterial replication properties of DNA-gyrase and topoisomerase IV (Thomas, 2008). Resistance is more difficult because it requires two mutations; however, there are documented cases of resistant bacteria species (Jhanji et al, 2007; Betanzos-Cabrera et al, 2009). Infections that appear more ominous may also be initially started on fortified aminoglycosides or cefazolin along with the empirical fluoroquinolone treatment (Forster, 1998).
If a patient was cultured, the treatment regimen may be altered based upon the known species and sensitivity reports. Acanthamoeba keratitis should be in the differential of any patient with known water exposure, for whom pain exceeds clinical appearance, or in cases that are not responding to antibiotics. Acanthamoeba are free living and exist as mobile trophozoites or dormant cysts. Diagnosis can be difficult, but can be accomplished with culture, biopsy, confocal microscopy, and identification of Acanthamoeba DNA by polymerase chain reaction (PCR). Initial misdiagnosis delays appropriate therapeutic management, which can worsen prognosis. Historically, topical biguanides, broline, aminoglycosides, or miconazole have been used therapeutically. However, biguanides may be the only effective therapy for the resistant encysted form (Dart et al, 2009). Resolution may take six months or longer.
There is some debate in the literature about using adjunctive topical steroids for the treatment of bacterial or Acanthamoeba MK. Destruction and scarring during MK events partially comes from the infectious organism, but it is also due to secondary inflammation. If you subscribe to adjunctive steroid treatment, add them to the therapeutic regimen once there is some improvement and reepithelialization (Cohen, 2009). However, there is a significant risk that topical steroids may enhance an infection secondary to steroid-induced immunosuppression. (Hindman et al, 2009). A similar debate previously occurred concerning using topical steroids to treat herpes simplex stromal keratitis, and the Herpetic Eye Disease study eventual found them to be safe and effective for stromal herpetic disease (Wilhelmus et al, 1994). A similar study is needed to determine whether adjunctive topical steroids would be safe and effective.
Fungal MK is rare, and as with Acanthamoeba keratitis, it is often misdiagnosed during its initial presentation. A fungal ulcer should be considered in any MK that is unresponsive to initial therapy. Natamycin, amphotericin, and voriconazole are all topical therapeutic options, although Natamycin is most commonly prescribed (Loh et al, 2009). Fungal keratitis can be slow to heal and may take months of therapeutic management before resolution.
Although silicone hydrogels and daily disposables have not demonstrated that they can decrease the incidence of MK, vision loss secondary to severe MK is less likely to occur with daily disposable contact lens wear (Dart et al, 2008; Stapleton et al, 2008). There is future potential to apply antimicrobial technology to contact lenses in an attempt to reduce the incidence of contact lens-related MK. Researchers are working on antimicrobial additions that would either be applied to the lens surface or incorporated into the lens polymer to prevent bacterial colonization or biofilm formation, both of which can lead to MK. These additives would have to be nontoxic, have a broad spectrum of antimicrobial activity, and have minimal impact on normal ocular flora (Gabriel and Weisbarth, 2009).
Conclusion
It had been expected that silicone hydrogels and daily disposable contact lenses would reduce the risk of contact lens-related complications. Silicone hydrogels have reduced the risk of hypoxia-related complications such as hyperemia and neovascularization, while daily disposables have reduced hypersensitivity/toxicity and CLPC complications (Donshik, 1994; Radford et al, 2009). However, neither of these advances has reduced the overall risk of acute nonulcerative contact lens complications, nor have they reduced the incidence of MK (Dart et al, 2008; Radford et al, 2009).
Correctly diagnosing these complications on initial presentation can be difficult because signs and symptoms of contact lens-related complications can broadly overlap. A careful history, examination, and detective work will help you improve your speed and accuracy of diagnosis, and with sound management you can return your patients to comfortable and safe contact lens wear. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #172.