


CONTACT LENS EVALUATION
Going Green to Evaluate Contact Lens Fit
Adding lissamine green conjunctival staining to a lens evaluation can shed light on lens fit and ocular health.
By Renee J. Garofalo, OD, FAAO, & Alison Carter Ramsey, OD, MS, FAAO

Dr. Garofalo is associate director of Consumer Products Clinical Trial Management with Alcon Research responsible for clinical research on new lens care products. Prior to joining Alcon, Dr. Garofalo was research optometrist for Wesley Jessen, served as adjunct professor at the Illinois College of Optometry, and was a scientific reviewer for the NIH. 
Dr. Ramsey is a clinical trial manager for Alcon Research, Ltd. She is a fellow of the American Academy of Optometry and a member of the American Optometric Association. |
Recent studies have shown that silicone hydrogel (SiHy) lenses may be associated with conjunctival staining (Maldonado et al, 2004; Meadows et al, 2009), mucin ball formation (Tan et al, 2003), diverse bacterial adhesion (Henriques et al, 2005; Kodjikian et al, 2008), and a higher frequency of corneal infiltrates when compared to traditional hydrogel lenses (Stapleton et al, 2008). Due to the higher modulus of some SiHy materials, the fit may be less forgiving than with a traditional hydrogel lens and may magnify any impact of the lens edge design (Woods, 2007; Løfstrøm, 2005).
In our clinic, we have anecdotally observed the unique ocular fit and lens material issues associated with SiHy lenses. Patients typically present for a routine exam wearing their current habitual lenses and using either a multipurpose or a peroxide-based disinfecting solution. As part of our standard contact lens evaluation, we document the lens age, wear time on day of examination, and lens fit (centration, lens movement in central and up gaze, and push-up test) in each patient's record.
In addition, we conduct a slit lamp examination and a corneal evaluation using fluorescein. Although typically applied to evaluate complaints of dryness, evidence in the literature suggests that lissamine green can also be used to detect conjunctival changes associated with contact lens wear (Begley et al, 1998). Therefore, we now evaluate conjunctival health with lissamine green. Conjunctival surface staining provides valuable information about fitting behavior that may have otherwise been missed.
Case Study 1
Our patient, an experienced contact lens wearer, presented for a routine contact lens aftercare visit with a history of 8.6mm balafilcon A (PureVision, Bausch + Lomb) lens daily wear cared for using Clear Care (Ciba Vision). He reported a feeling of deposit buildup in the left eye. During slit lamp exam, the lens moved optimally and centered well. Application of lissamine green to the bulbar conjunctiva revealed no lens edge/limbal staining. However, the conjunctival folds displayed excessive pooling (Figure 1).
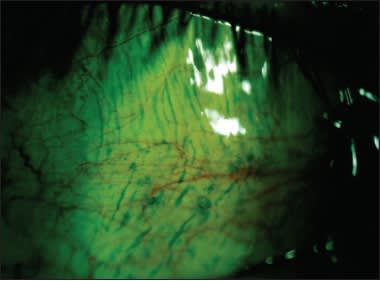
Figure 1. First case study patient's bulbar conjunctival staining.
To address the deposition issue, we dispensed Opti-Free Replenish (Alcon) multipurpose solution and a new pair of lenses. At subsequent office visits over the following weeks, we determined that the change in lens care solution addressed his primary concern.
Case Study 2
A patient presented at the initial clinic visit wearing 8.4mm senofilcon A (Acuvue Oasys, Vistakon) lenses on a biweekly replacement schedule and using Opti-Free Replenish. She was asymptomatic, the lens exhibited minimal movement (tight lens fit), and the bulbar conjunctiva displayed marked lens edge staining with lissamine green.
To rule out the possibility that a solution/lens interaction was causing the lens edge staining, we changed her solution to Opti-Free Express (Alcon) multipurpose solution at the second visit, and then to Clear Care at the third clinic visit, dispensing new 8.4mm senofilcon A lenses at each visit. The circumlimbal conjunctival staining was present with each care solution/contact lens combination, eliminating the solution as the cause. We advised her to continue using Clear Care and dispensed the flatter 8.8mm senofilcon A lens.
At the follow-up exam, the circumlimbal conjunctival staining was still evident (Figure 2). Therefore, we prescribed lotrafilcon A (Air Optix Night & Day Aqua, Ciba), which has a different edge design. We gave her a new pair of lenses and Clear Care and asked her to return to the clinic in three days. On follow up we found that by changing the lens, the circumlimbal lissamine green conjunctival staining had resolved.

Figure 2. Case study two patient's circumlimbal lissamine green staining.
A Careful Evaluation
Since adding lissamine green conjunctival staining as part of our standard contact lens evaluation, we have observed that most patients wearing a SiHy lens exhibit varying degrees of contact lens-induced conjunctival staining (CLICS). The CLICS observed with lissamine green stain may be indicative of a poor lens fit or edge design.
Given that chronic mechanical trauma may be associated with additional clinical findings, including infiltrates (Catania, 1995 [a]); Catania, 1995 [b]) and conjunctival epithelial flaps (Løfstrøm, 2005; Hubner et al, 2009), we now methodically refit patients exhibiting CLICS into new contact lens/care solution combinations until one is identified that minimizes conjunctival staining. Depending on the initial observations, we make changes to the contact lens/care solution combination one parameter at a time. We change only one parameter such as a base curve, lens material, or care solution between any two given office visits. We schedule visits approximately three days apart to allow for ample lens equilibration.
Changes in care solutions, whether multipurpose or peroxide-based, have not had an effect on the circumlimbal conjunctival staining observed in our patients. However, changes in lens parameters and lens materials have had a measurable impact on the reduction of circumlimbal conjunctival staining. Therefore, our experience suggests that much of the circumlimbal conjunctival staining may be more of a lens fit issue rather than a care solution interaction.
When a patient presents to your practice with an adverse event related to contact lens wear, evaluate the entire ocular health to identify the root cause(s) before arbitrarily changing the current care regimen. After two major recalls of marketed contact lens care products, and with the understanding that there can be decreased levels of biocompatibility with certain contact lens/care solution combinations (Andrasko, 2008), practitioners now more often assume that contact lens complications are care solution-related. Before making the call, step back, take a good case history, and adequately assess lens fit.
• Ensure that the patient has been compliant with the recommended lens care regimen and wearing schedule.
• Make sure the ocular surface, tear film, and lid margins are otherwise healthy.
• Soft contact lenses may tighten with wear, causing the lens to be less noticeable to the wearer, and should be evaluated after the lens has had adequate time to equilibrate (Meadows et al, 2009). Re-assess the fit at least 20 to 30 minutes after application and again in the afternoon after the patient has worn the lenses for several days. The lens needs to have optimal movement to prevent the post-lens tear film from becoming stagnant and developing mucin balls. The tear film should be able to flush properly to allow cellular debris, biochemical components, and bacteria to escape from behind the lens.
• Use fluorescein stain when assessing corneal health. Localized staining in only one or two corneal or limbal zones may indicate desiccation or a mechanical issue, while diffuse bilateral corneal staining may indicate solution sensitivity.
• Use lissamine green to assess conjunctival health. Conjunctival staining associated with tight lenses or lens edge designs that hug the limbal area may suggest either a poor lens fit or lens edge design.
Conclusion
Adding lissamine green to your contact lens examination will provide valuable insight into lens fit and the overall health of the ocular surface. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #174.