


prescribing for presbyopia
How Much Add Power is Enough?
BY CRAIG W. NORMAN, FCLSA
How do we determine what add is best for individual patients? Is it simply their spectacle add power—or do we need to make additional adjustments to provide the best range for the various needs that each patient has throughout the day?
Let's look at how this is best managed among the three categories of presbyopic patients that we encounter (Table 1).
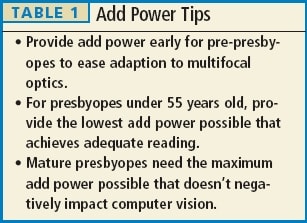
Pre- or Emerging Presbyopes
More and more practitioners today are recommending an add power in contact lenses for younger presbyopic patients. The rationale here is twofold. One, myopic patients experience earlier presbyopic symptoms while wearing spectacles. Two, there is a sense that if a patient can begin the adjustment to more complex multifocal optics while they still have strong accommodative function, then it will be easier for them to adapt, especially in simultaneous vision designs.
So when should you consider these designs? From my perspective, as soon as a patient describes any decrease in reading function, consider a lens that provides multifocal optics. This strategy has changed over the years. In the past I would hold off as long as possible from trying to correct a presbyopic patient with contact lenses only, but now with so many habitual soft lens wearers reaching presbyopia I've modified this approach.
Under-55 Presbyopes
Presbyopes wearing soft lenses usually see best at all levels with the least amount of add power provided within a design. For lenses that are available in only two add parameters, keep patients in the low add for as long as possible. Even when this is no longer functional, consider changing only one (usually the nondominant) eye to the higher add power first.
For lenses that have multiple add power options, make changes incrementally in 0.25D steps whenever possible.
Do not over use higher add powers in this patient group. Also, don't try to measure the effectiveness of these add power changes within a few minutes in the office. Instead, allow these patients to wear diagnostic lenses over a period of days to better determine the effectiveness of add power changes.
Mature Presbyopes
For patients over 55, the story is a little different. While I generally try to follow the "lowest add power" adage described above, for mature presbyopes I have concern with the intermediate (computer) vision. The increased use of smartphones has made this vision level a challenge for these patients.
So, for mature presbyopes I maximize the add power until the change has impacted patients' vision at the computer level.
Aiming for Two Out of Three
In this column I often refer to the "two out of three" philosophy, in which I ask patients to choose which two of three levels of vision—reading, computer, and driving—are most important to them, then ensure that we correct their choices as best as possible.
Controlling (minimizing) the add power goes a long way toward achieving that goal. CLS
Craig Norman is director of the Contact Lens Section at the South Bend Clinic in South Bend, Indiana. He is a fellow of the Contact Lens Society of America and is an advisor to the GP Lens Institute. He is also a consultant to B+L.