


treatment plan
More Options for Treating Retinal Vein Occlusion
BY LEO SEMES, OD, FAAO
In my last column, I discussed the results of two controlled clinical trials comparing intravitreal triamcinolone to standard care for central and branch retinal vein occlusion (RVO). Included was the FDA-approved Ozurdex (Allergan), an intravitreal sustained implant. Here we'll discuss the ever-widening off-label application of anti-vascular endothelial growth factor (VEGF) agents to treat RVO.
Studies and Results
Within the last year, there has been enormous progress in restoring vision for patients who have macular edema secondary to RVO. Macular edema may be a difficult entity to appreciate clinically. While this may be more complicated in cases of diabetic macular edema and clinically significant macula edema, sudden painless vision decrease may be a distinct symptom. While this is non-specific to macular edema or RVO, the clinical picture of RVO is usually dramatic.
Recently, the six-month results were released of a clinical trial comparing an intravitreal injection of the anti-VEGF agent ranibizumab (Lucentis) for macular edema in patients who have central or branch RVO. Interim positive results also were reported recently from an industry-sponsored study.
The BRAVO (A Study of the Efficacy and Safety of Ranibizumab Injection in Patients with Macular Edema Secondary to Branch Retinal Vein Occlusion) and CRUISE (A Study of the Efficacy and Safety of Ranibizumab Injection in Patients with Macular Edema Secondary to Central Retinal Vein Occlusion) ongoing studies are sponsored by Genentech, manufacturer of Lucentis (ranibizumab). Both studies are designed to investigate the safety and efficacy of drug intervention (0.3mg or 0.5mg intravitreal injection) versus treatment with a sham procedure. The trials include nearly 400 patients in each study.
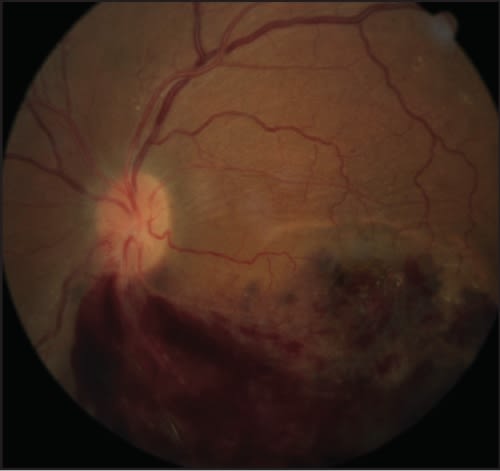
Figure 1. Branch retinal vein occlusion with severe macular edema. The patient was offered treatment with intravitreal bevacizumab.
The six-month results demonstrated 15-letter improvement in 74/134 (55.2 percent) eyes in BRAVO for the 0.3mg dose, while 80/131 (61.1 percent) eyes showed the same improvement with the 0.5mg dose. Average gain for all treated eyes was just more than seven letters while the sham group showed a mean 1.9 letter improvement. For eyes in CRUISE, 61/132 (46.2 percent) and 62/120 (47.4 percent) showed 15-letter improvement in response to the 0.3mg and 0.5mg doses, respectively.
For clinical comparisons, each five-letter increment is roughly equivalent to a line of visual acuity. The average gain in the sham group was only 1.1 letters. Note that the comparison group received sham injections. From this we can conclude that the natural course of the macular edema is minimal improvement.
Treatment Options
We should be aware of treatment options and encourage patients to take advantage of modalities provided by retina specialists. We should also consider the results of the CRUISE and BRAVO trials and the off-label use of the tested anti-VEGF agent. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #174.
Dr. Semes is a professor of optometry at the UAB School of Optometry.