


TORIC OPTIONS
Choosing the Right Toric Option
A case study highlights how you can help astigmats on their quest for clarity.
By Thomas G. Quinn, OD, MS, FAAO

Dr. Quinn is in group practice in Athens, Ohio. He is a diplomate of the Cornea and Contact Lens Section of the American Academy of Optometry, an advisor to the GP Lens Institute, and an area manager for Vision Source. He has served as an advisor or consultant to CooperVision, Ciba Vision, and Vistakon and has received research funding from AMO, B&L, Ciba Vision, CooperVision, and Vistakon. |
The days of turning away astigmatic patients who are interested in the many benefits of contact lens correction are gone. Let's look at the case of a patient in the first-person account below and explore what contact lens option might best meet his goals. You'll find that there might be more than one answer.
A Quest for Freedom and Clarity
"Name?" queried the stern library clerk.
"Matt. A. Stieg Matt," I replied. "My friends call me Stieg," I quipped, hoping for a smile.
I was answered with a scolding raised right eyebrow. She just didn't get me. Many people don't.
All my life people have mispronounced my name, tried to mask my presence, mostly without success, or simply turned me away. "Sorry, Mr. Matt. We can't help you." I was determined to twist this all-too-familiar story line. Flip it on its axis.
I am a man of diverse interests. A 39-year-old journalism professor, I do a fair amount of traveling and speaking, in addition to my regular duties in the classroom. When I'm not on the road, I often spend days at a time on the computer, researching a wide array of interests. It can be pretty intense work, so I try to find some balance by exercising at least four days a week. When weather permits, I like to kick-start my day with a morning jog. The cold winter months find me trying to keep up with the younger guys on the basketball hardwood. When my body says it's had enough, I enjoy sauntering through the woods with my trusty binoculars, bird watching.
With the exception of some springtime allergies, I�m in excellent health. Throw in my talented, beautiful wife and two fabulous kids, and it all adds up to a pretty good life.
But I know it can be better. Contact lenses would offer me great freedom from my sweat-splattered, heavy-rimmed sport goggles. Call me vain, but I'd love to shed my spectacles when I present myself before an audience of students or peers.
Entering the library, all I had was a piece of paper with results from my last examination:
Refraction: OD −2.00 −1.00 x 180 20/20 (dominant eye) and OS −1.00 −2.75 x 180 20/20.
Keratometry: OD 42.25 @ 180; 44.75 @ 090 and OS 42.00 @ 180; 44.75 @ 090.
As I emerged from the great hall of information, I felt I had crossed into a new world, a world aligned with my vision. With renewed hope, I set out to find a provider who could help me realize my quest; a quest for freedom and clarity.
Soft Perspective on the Right Eye
Using Mr. Matt's case as an example, let's look at the options that will help him—and many of our other patients—on their quest for clarity.
Mr. Matt's right eye has corneal astigmatism that does not match the astigmatic refractive error. Because a firm lens would create a 2.50D astigmatic tear lens when only 1.00D is needed, it is reasonable to consider a soft lens as the best option.
Although some may be inclined to start by applying a spherical soft lens to an eye with 1.00D of astigmatism, it has been shown that masking this degree of astigmatism is successful less than 17 percent of the time (Snyder and Talley, 1989). Additionally, studies have repeatedly demonstrated that patients with this degree of astigmatism note significantly improved vision with a toric soft lens when compared to spherical soft lens correction (Richdale et al, 2007; Bayer and Young, 2005). The fact that, in our case, the right eye is the dominant eye, makes it even more compelling to provide full visual correction of the refractive error.
Concerned about time and ease of fit? Bayer and Young (2005) found this degree of astigmatism can be corrected efficiently and effectively with a toric soft lens. In their study, patients in this astigmatic range were successfully fit with the first lens dispensed in 91 percent of cases.
Daily Disposable Toric Soft Lenses
Mr. Matt's ability to wear his contact lenses may be impacted by his seasonal allergies at springtime. Applying a fresh, clean lens every day may provide the best performance during this time of year. Daily disposable toric soft lenses are offered in an everwidening range of cylinder powers and axes.
CooperVision's ClearSight 1 Day Toric, available in −0.75D and −1.25D of cylinder power, is offered in four axes (Table 1). CooperVision's historical lens-ordering data suggest that these parameters allow 84 percent of patients whose axes fall within 10 degrees of either side of each axis to be fit successfully (CooperVision Data on File). This lens utilizes the same stabilization design as the rest of CooperVision's line of torics, which are based on the prismballasted design of the Biomedics Toric.
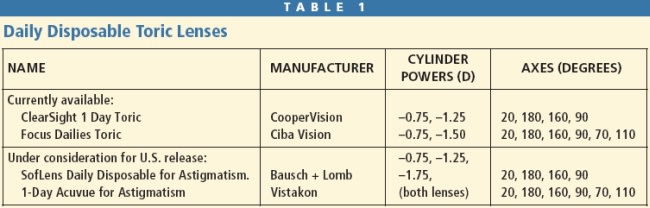
Ciba Vision's Focus Dailies Toric, the first daily disposable toric on the market in the United States, has expanded the available axes from the original 90 and 180 degrees to include 20 degrees on either side of these axes, which is very beneficial. A cylinder power of −1.50D is now offered in addition to the original cylinder power of −0.75D. The higher the cylinder power, the more critical it is to have appropriate alignment with the axis of the astigmatic refractive error (Linksz, 1942).
Both Bausch + Lomb and Vistakon are evaluating release of a daily disposable toric in the United States. B+L's SofLens Daily Disposable Toric employs the same material and aspheric optics found in its spherical daily disposable lens, as well as the Lo-Torque prism-ballasting geometry employed by its entire line of toric lenses. Vistakon's 1-Day Acuvue for Astigmatism is fabricated in the 1-Day Moist material. It is stabilized using the Accelerated Stabilization Design featured in its line of toric lenses. Although daily disposables are an attractive option for Mr. Matt's right eye, current power limitations make it less likely to satisfy the visual needs of the highly astigmatic left eye.
Soft Perspective on the Left Eye
When selecting a soft toric for the left eye, should the lens of choice be a hydrogel or silicone hydrogel toric? All toric lenses have areas of increased lens thickness built into their design in an attempt to prevent lens rotation. This greater thickness may increase the difficulty of providing the underlying corneal tissue with adequate levels of oxygen. Brennen (2008) has found less corneal stress induced with wear of silicone hydrogel toric lenses versus hydrogel torics under both open and closed eye conditions.
Another reason to consider a silicone hydrogel toric lens as the preferred option is the belief that these lenses may stabilize on the eye more rapidly. This may be due to new stabilization designs, the fact that silicone hydrogel materials do not dehydrate as much as hydrogels do (Jones et al, 2002; Morgan and Efron, 2003), or a combination of both of these factors. The newest addition to the silicone hydrogel toric family is the Avaira Toric (CooperVision). This lens is made of the same material as the Avaira sphere lens and utilizes the Biomedics Toric design, as does its Biofinity Toric lens.
However, currently all available silicone hydrogel toric lenses have cylinder power limited to −2.25D. Many toric hydrogel soft lenses are offered to correct up to and beyond the 2.75D of astigmatism required to correct the refractive error in Mr. Matt's left eye.
Do the current power limitations of silicone hydrogel torics rule them out as a viable option for the left eye?
Soft Toric Power Considerations
When prescribing any toric soft lenses, strive to provide clear vision with the lowest cylinder power that will do the job. Why? The higher the cylinder power, the greater the visual disturbance with any lens mislocation (Linksz, 1942).
Would a −2.25D toric power be adequate to provide Mr. Matt with good vision on his 2.75D astigmatic left eye? One way to determine this is to modify the final spectacle power in the phoropter to −2.25 and adjust the spherical component to see if adding minus improves clarity. Bergenske (2003) has shown that this method provides a good assessment of what visual performance will be when a properly fitting toric lens of this power is applied to the eye.
If this demonstration provides good vision, a silicone hydrogel toric might be the best approach to take with the left eye. If vision was not adequate, we have the option of a −2.75D cylinder hydrogel toric or a GP lens.
A study of 19 subjects who had astigmatism of −2.50D to −5.00D found that 14 subjects (74 percent) preferred the vision of GP torics and 11 subjects (58 percent) chose to continue to wear GP toric lenses at the completion of the study (Michaud et al, 2009). Of the eight subjects choosing to continue to wear soft torics, six had been soft toric wearers prior to the study.
You might reasonably conclude that a GP toric design on the left eye is the best choice, particularly since Mr. Matt has no prior experience with either form of contact lens correction and participates in the visually demanding activity of bird watching.
Fitting a GP Toric
For decades, astigmatic patients have been well served by firm lenses, dating back to PMMA "hard lenses" up to today's sophisticated line of oxygen transmitting GP lenses.
When refractive cylinder is equal to and aligns with corneal cylinder, a simple spherical GP lens can be employed to correct both spherical and astigmatic refractive error. If corneal toricity is in the range of 2.00D or more, a toric GP may be needed to provide a stable fit and clear vision (Figures 1 and 2).
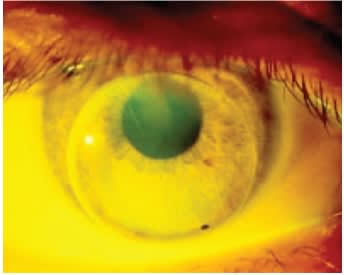
Figure 1. Poorly fitting spherical GP on a 3.00D toric cornea.

Figure 2. Well fitting toric GP on the same 3.00D toric cornea.
GP Toric Versus Soft Toric
When considering a GP toric lens, many practitioners get bogged down by attempting to determine at the outset what type of toric GP (such as bitoric, back toric, etc.) will be needed in a given case. Described here is a process in which an ideal fit is designed, after which the needed powers, and therefore toric type, are derived as the final step.
Diameter is First The first parameter to choose when designing a toric GP is diameter. I'll explain why shortly.
Many factors should be considered when making this decision, such as aperture size, pupil size, and horizontal visible iris diameter. Simplify this process by focusing on the position of the upper eyelid margin relative to the superior limbus. If the eyelid covers the superior limbus, select a large overall diameter (e.g. 9.5mm). This will allow you to tuck the superior lens edge under the upper eyelid, commonly referred to as a lid-attachment approach. With this approach, the upper eyelid does not need to blink over the lens edge, enhancing comfort.
If the eyelid margin rests above the upper limbus, you should strive for an interpalpebral fitting relationship, choosing a smaller overall diameter (e.g. 8.5mm). In Mr. Matt's case, let's say his upper eyelid margin covers his upper limbus, so we will attempt a lid-attachment fit with a 9.5mm overall diameter.
Selecting the Base Curve Radii Putting toric GP lenses aside for a moment, if fitting a spherical GP, what corneal characteristics would be ideal to achieve a good fit? Many would agree that some corneal toricity would be desirable. A spherical lens on a perfectly spherical cornea will often not move well. With-the-rule corneal toricity would promote movement in the vertical direction, in harmony with the eyelids during the blink. Toricity of 0.75D may be the ideal amount, as it has been shown that there is some risk of lens flexure when toricity exceeds this amount (Harris and Chu, 1972).
In summary, the ideal cornea onto which to fit a spherical GP lens would have �0.75D of with-therule toricity. So, when designing a toric GP lens, choose a base curve radius in the horizontal meridian that results in a near alignment fit and a base curve radius in the vertical meridian that is 0.75D flatter than what is done horizontally. This will mimic the ideal fit of a spherical GP lens on a slightly with-therule cornea.
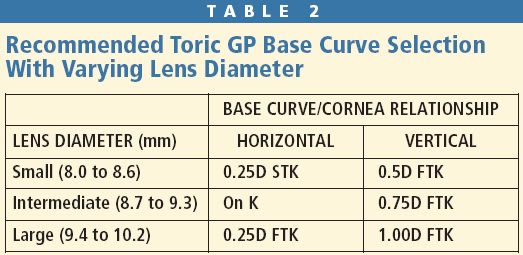
Size Matters When Choosing Base Curve Radii At this point in the design process, diameter must be factored into the base curve selection. A larger contact lens will vault more, or have more sagittal depth, than would a smaller contact lens of the same base curve radius (Figure 3). So, when fitting a larger diameter, a flatter base curve radius is needed to achieve desired clearance. Conversely, when a smaller diameter is chosen, a relatively steeper base curve radius is needed to achieve the same sag. Table 2 lists suggested base curve radii selections for various overall diameters.
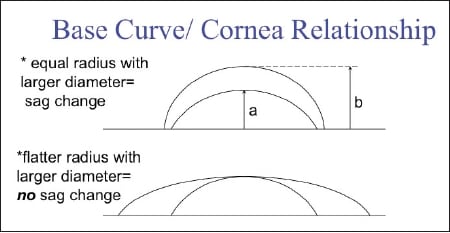
Figure 3. Effect of diameter on sagittal depth.
Once base curve radii have been chosen, factor in tear lens effects to arrive at lens power in each meridian. Figure 4 shows the derived lens parameters for Mr. Matt's left eye.
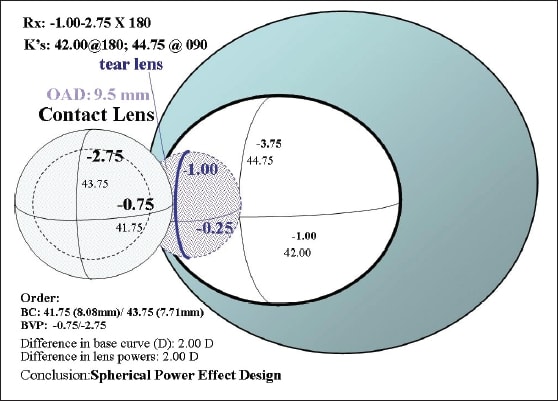
Figure 4. Derived lens parameters for Mr. Matt's left eye.
Figuring Out GP Toric Type
Although we have the information necessary to order a toric lens for Mr. Matt's left eye, one more step is necessary to arrive at the design. That step is to compare the difference between the two base curve radii (in diopters) to the difference in lens power between the two major meridians. In our case, these two values are equal:
Difference in base curves = 43.75D − 41.75 = 2.00D
Difference in powers between major meridians = 2.75D − 0.75D = 2.00D
When these two values are equal, we have a spherical power effect (SPE) design (Sarver, 1963). This means the lens can rotate without disturbing vision. Whenever the corneal toricity matches the spectacle astigmatic error—a common scenario—a SPE design will be derived and lens rotation will not be a concern.
If the difference in base curve does not equal the difference in powers, you will be working with a cylinder power effect (CPE) design, and any lens rotation will cause blur. In this case, take the following precautions:
1. Make sure there is at least 2.00D of toricity in the base curve.
2. Make sure the base curve toricity is at least two-thirds of the corneal toricity.
Both of these precautions are to ensure that there is enough toricity in the base curve for the lens to lock into place (Quinn, 1999).
GP Perspective on the Right Eye
Although an SPE toric lens may be a good option for Mr. Matt's left eye, how does the GP option look for the right eye? A toric GP is an option for this eye as well, but a CPE design would be necessary, and concerns about rotation exist.
There is another possible GP option: a flexing GP lens.
As stated earlier, a non-flexing GP lens on the right eye will induce an astigmatic tear lens of 44.75D − 42.25D = 2.50D. The patient's refractive error calls for only 1.00D of astigmatic correction. If a lens could be designed to flex while resting on the corneal surface, the astigmatic tear lens would be diminished.
You can promote flexure by reducing center thickness, steepening the fit (Herman, 1983), and choosing a higher-Dk material. Higher-Dk materials tend to have a lower modulus, making them more flexible (Szczotka-Flynn, 2005).
The Hybrid Option
A firm center/soft skirt contact lens, such as the SynergEyes A (SynergEyes, Inc) lens design, may be an option in Mr. Matt's case. It is difficult to know whether such a lens would flex enough for the right eye and resist flexure sufficiently for the left eye. Specifying an enhanced profile (EP) lens design, adding to the center thickness of the firm portion of the lens, would help reduce flexure of the left lens.
The Preferred Option?
Soft contact lenses offer better initial comfort and a simpler, and therefore perhaps more predictable, approach for the dominant right eye. GP contact lenses may offer better vision, particularly in the highly astigmatic left eye. An additional benefit to GP lenses and hybrid lenses would be the ability to perhaps more easily transition into a multifocal design when presbyopia develops.
Conversing with your patients will give you an understanding of their priorities and can guide you to the best approach as you assist them with their quest for freedom and clarity with contact lens correction. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #178.