


GP Insights
A New Corneo-Scleral Lens Option

By Ann Laurenzi-Jones, OD, FAAO
The Perimeter Lens by Essilor is a corneo-scleral lens with a large overall diameter (OAD) of 14.00mm to 14.80mm. The lens was designed to fit regular and irregular corneas when a corneal GP lens will not work, the vision provided by a soft lens is less than adequate, or if the patient is unsuccessful with a hybrid lens. The Perimeter may fill in gaps where other lenses fail.
The large OAD may have you thinking that it is fit like a scleral lens in which the entire cornea is vaulted and the weight of the lens rests solely on the sclera. Different from a scleral lens, the properly fit Perimeter lens distributes the weight of the lens between the cornea and sclera (Figure 1). The central fitting zone is designed to align with the central cornea. The lens achieves the alignment fit with a central optic zone and two additional curves (base curves 1, 2, and 3) that flatten out to the limbus. The base curves are followed by a pivotal curve that vaults the limbal area, the same as a scleral lens. The peripheral curves of the lens form a support curve that lands on the sclera and bears the remaining weight of the lens, followed by a peripheral curve that allows for tear flow under the lens.
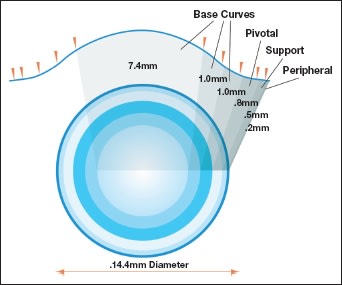
Figure 1. The Perimeter lens elevation map.
Fitting Tips
When fitting the Perimeter lens it is critical to observe the peripheral and support curves first, and then move inward to adjust the remaining curves.
After determining the base curve (mean K or average of simulated K readings from topography), place a diagnostic lens on the eye. The fluorescein pattern determines whether the support curve aligns with the sclera. For example, lift off (or edge lift) of the lens support curve or peripheral curve would mean the base he Perimeter Lens by Essilor is a corneo-scleral lens with a large overall diameter (OAD) of 14.00mm to 14.80mm. The lens was designed to fit regular and irregular corneas when a corneal curve is too flat. This is one of the most common fitting errors.
If you see touch in the horizontal meridian (like parentheses nasal and temporal to the limbus) the support curve may be bearing too close to the limbus. This means the OAD is too small and should be increased to correct the fit. If the support curve pools fluorescein at its inner edge, flatten it to achieve alignment.
The support curve does not change sagittal height, but the pivotal curve does. The pivotal curve should not bear any weight on the limbal area. This is crucial to long-term success. Bearing in the limbal area can damage stem cells and reduce oxygen supply to the cornea by compressing blood vessels and lessening blood flow. If you see bearing in the limbal area, steepen the pivotal curve. Changing the pivotal curve or the OAD requires a compensating change in the base curve to keep the sagittal height the same.
Lastly, check the base curves to ensure there is no excessive corneal bearing or vault. Because the lens has a larger diameter, most find it very comfortable.
The lens is manufactured in Boston XO or XO2 (both Bausch + Lomb). Both provide superior optics and hyper oxygen transmissibility to maintain the health of the eye. CLS
Dr. Laurenzi-Jones currently has a staff position at NorthShore University Hospital in Glenbrook, Illinois. You can reach her at annlaurenzi@yahoo.com.