


REFRACTIVE SURGERY
The Technology Behind Refractive Surgery
Technological advancements in pre-surgical and surgical instrumentation are improving safety and outcomes.
By Marc Bloomenstein, OD, FAAO

Dr. Bloomenstein is the director of Optometric Services at the Schwartz Laser Eye Center in Scottsdale, Ariz. He is a founding member and current president of the Optometric Council on Refractive Technology and is an adjunct assistant professor at the Southern California College of Optometry. He has served as an optometric advisor to Staar Surgical, B+L, Allergan, Odyssey, Inspire, TearLab, and Alcon. |
Consider the technology that is in common use today, including cell phones with numerous applications, music players, portable readers, and computers. This onslaught of new ideas and technology is not lost on our precious eyes: silicone hydrogel contact lenses, wavefront-correcting lenses, and enhanced progressive lenses dominate the ophthalmic landscape.
The progress that we see in ophthalmic lenses is mirrored in the advances observed within refractive technology. Although the processes may stay constant, the end results are safer, more efficacious, and can provide patients with the quality expected in this day and age.
Preparing the Ocular Surface
Yet, like a chain, it is only as strong as the weakest link. Refractive surgery is only as good as the surface of the eye.
Our profession was founded on the clear principle of providing an excellent refractive outcome. However, without a healthy refractive surface, our visual efforts are thwarted by persistent inflammation. Fortunately, the most common side effect of refractive surgery—dry eye—can be minimized with pretreatment and education.
Ocular surface inflammation may often present as an obstacle to achieving the best result, and must be treated appropriately. Therefore, a thorough evaluation of the lid margin, tear volume, corneal surface, conjunctiva, and finally, the retina, is critical. Evidence of any lid disease, even asymptomatic, warrants treatment. Any patient who is self-medicating with artificial tears should be classified as symptomatic.
New technologies approved by the U.S. Food and Drug Administration (FDA), such as the TearLab Osmolarity Test (TearLab Corp., Figure 1), may alleviate some of the diagnostic quagmire. With a sample taken from one tear, the TearLab can provide instantaneous osmolarity results and information about a patient's ocular surface environment. The benefit of this new equipment is that it provides a diagnostic marker that has been defined by the Dry Eye Workshop (DEWS) as a component of dry eye.

Figure 1. The TearLab Osmolarity test can provide instant osmolarity results from a single tear.
The use of lid hygiene scrubs and warm compresses should become more standard practice. Artificial tears may provide some relief, but the palliative nature of these drops leaves your patients in a vicious cycle. The inflammatory nature of dry eye and lid disease was brought forth almost two decades ago. If a patient is already self-medicating with artificial tears, consider treating with cyclosporine and more aggressive artificial tears. A hydrated cornea has been associated with improved visual outcomes and reduced inflammation in both contact lens patients as well as in refractive surgery patients. Likewise, treating the lid margin before any refractive surgery procedure is beneficial. It has long been established that tetracycline derivatives help improve posterior blepharitis. Now we have seen clinical evidence that topical azythromycin has the same effects on posterior blepharitis.
Recent studies (Foulks et al, 2009; Zhou et al, 2009) have shown that the use of topical azythromycin has the same clinical benefit without the systemic side effects. I prefer to start my treatment topically, but I switch to oral azythromycin for recalcitrant blepharitis. The key is that we must be aggressive in treating the lids prior to any new technology. Thus, you must evaluate any refractive surgery candidate in the office prior to surgery.
Moreover, you need to follow your patients before you can refer them for surgery. These medical follow-up visits are an important part of the doctorpatient relationship and result in the best refractive outcomes. Today we have some of the best new medical modalities including punctal plugs, nutraceuticals, and other topical treatments, which may need to be included at any time prior to, during, and after the surgical procedure. Scheduling the followup appointments allows you to evaluate whether your treatment is effective.
Technology has improved our ability to create a healthy refractive environment. So what is new with the surgical procedures? How has technology taken refractive surgery to the next level?
Laser-Assisted in Situ Keratomileusis (LASIK)
LASIK surgery remains the most prolific corneal refractive surgical procedure today. LASIK has proven through the years to be both safe and efficacious. In fact, almost everyone can undergo LASIK, yet not all patients will have the desired result. The advancements we have observed are in the ability to detect who is most likely an excellent candidate.
Reichert Technologies has introduced the Ocular Response Analyzer (ORA, Figure 2). The Reichert ORA employs a dynamic bi-directional applanation process to measure IOP and the biomechanical properties of the cornea. The ORA utilizes a rapid air impulse and an advanced electro-optical system to record two applanation pressure measurements, one while the cornea is moving inward, and the other as the cornea returns. Because of its complex viscoelastic structure, the cornea resists the dynamic force of the air pulse, causing a delay in the inward and outward applanation events, resulting in two different pressure values. The average of these two pressure values provides a repeatable, Goldmann-correlated intraocular pressure (IOP) measurement (IOPcc). The difference between these two pressure values is corneal hysteresis (CH). The CH measurement is an indication of viscous damping in the cornea, or the ability of the tissue to absorb and dissipate energy.
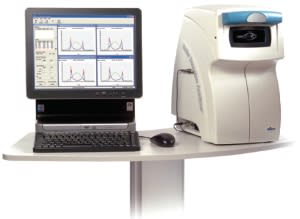
Figure 2. Reichert's ORA uses bi-directional applanation to measure IOP.
These new metrics may provide the elusive information needed to determine who will develop postsurgical ectasia, similar in appearance to keratoconus, prior to LASIK. Ectasia is arguably the most serious possible post-LASIK complication. Currently, we evaluate central corneal thickness and topographical appearances to rule out any patient who may potentially become ectatic. Yet, even when these factors are well within normal limits, patients have still developed the characteristic inferior steepening and decrease in vision associated with ectasia. Shimmyo et al (2004) compared corneal viscous damping (CH) and viscoelastic response to deformation (CRF) in normal eyes, keratoconic eyes, and pre- and post-LASIK eyes (206 normal, 60 keratoconic, 100 pre- and post-LASIK eyes). Their results indicate that CH and CRF were significantly reduced in both keratoconic eyes and in post-LASIK eyes.
Abbott Medical Optics has also been working on bringing the iDesign to market. The five-in-one equipment would provide aberrometry, topography, pupillometry, keratometry, and refractometry with a single push of a button. The iDesign has an 8.5mm corneal coverage, integrated iris registration as well as the highest resolution of Hartmann-Shack aberrometry. This will allow for detection of anomalies prior to surgery.
How this correlates to our patients is evident from an article in Consumer Reports. As reported, patients age 55 and older were the least likely to report laser-vision-correction surgery side effects, slightly surpassing patients age 40 and younger, according to a recent Consumer Reports survey of 793 adults who underwent one of these procedures in the past eight years. Furthermore, the survey showed that patients age 40 to 54 were at the greatest risk of post-operative side effects. These findings were a major deviation from all other survey data, which revealed—not surprisingly—that the younger the patient, the greater the likelihood of positive outcomes. Laser-vision-correction surgery patients younger than age 40 were the most likely to report improvements in their effectiveness at work as well as in sports and leisure activities. Consumer Reports editors theorized that doctors may be doing a better job of eliminating inappropriate candidates. We have also adopted refractive options that relate to our patients.
In the surgical suite, the use of femtosecond technology to create flaps has surpassed the microkeratome in both safety and usefulness. This past year, AMO released the fifth generation Intralase laser. The iFS Advanced Femtosecond Laser is capable of creating a corneal flap in less than 10 seconds. The newest iFS also creates an inverted bevel-inside cut angle designed to provide a safer and stronger flap, elliptical flaps, and full customization capabilities. This combined with the advancements in wavefrontguided LASIK surgery has helped establish a sense of consistency and limited side effects. Dry eye, the most common post-LASIK side effect, can be minimized with pretreatment and education.
Phakic Intraocular Lenses (IOLs)
Currently, the Visian ICL (Staar Surgical, Figure 3) is the only alternative viable refractive procedure to LASIK that helps to maintain superior outcomes. This phakic posterior chamber lens is inserted through a 2.5mm self-sealing corneal incision and has safely expanded our refractive surgical candidates' options. The lens can be fitted for a patient who has a refractive error as low as −3.00D; however, the best benefit is observed in patients who are outside of the safe parameters of LASIK—those with corneas that are too thin, topographies that are questionable or demonstrate irregularities, and patients who have exceptionally high myopic refractive errors.
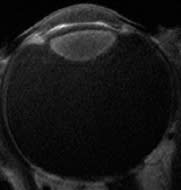
Figure 3. The Visian ICL is an alternative for poor LASIK candidates.
Although we can use a bioptic approach, combining technologies to treat astigmatic myopes, the FDA approval of the toric version of the Visian will ultimately benefit our patients. Sadly, we still do not have an FDA-approved hyperopic phakic IOL, and it is unlikely that we will in the near future. Young hyperopes often must continue to wear contact lenses and wait until presbyopia occurs to pursue an intraoperative surgical option.
Intraocular Surgeries
Refractive technology is not solely limited to treating the cornea. In fact, cataract surgeons have been accomplishing as much, if not more, with IOLs than what any excimer laser could perform.
Toric IOLs from Alcon and Staar Surgical have established a viable option for astigmatic reduction. Toric IOLs are expanding and thus creating opportunities for topographically challenged patients as well as for simply reducing a highly astigmatic eye.
The use of toric IOLs and the use of limbal relaxation incisions now can be improved with the introduction of the ORange (WaveTec Vision, Figure 4). This intraocular wavefront analyzer provides a realtime evaluation of sphere, cylinder, and axis in a matter of seconds. As small and compact as the ORange is, the large dynamic range (−5.00D to +20.00D) exceeds that of office-based wavefront aberrometry systems. Conventional wavefront technologies such as Shack-Hartmann are capable of measuring refractive power in a limited dynamic range, typically from −10.00D to +8.00D. The ORange uses Talbot-Moiré interferometry, which has a wider range of effective measurement compared to Shack-Hartmann and maintains a high resolution throughout its wide dynamic range. As a result, the aberrometer can accurately measure aphakic eyes intraoperatively, which promotes more accurate IOL power calculations particularly in eyes that have undergone refractive surgery. Current applications of the ORange include measuring limbal relaxation incisions, guiding their placement, and ensuring the accurate positioning of toric IOLs. By the end of this year, the addition of a hyperopic lens to the aberrometer will enable surgeons to perform on-the-table IOL calculations in an aphakic eye.

Figure 4. WaveTec Vision's ORange intraocular wavefront analyzer features a large dynamic range.
Presbyopia Options
You need to look no further at how far we have come with refractive technology than the advances in presbyopia correction. With each year that passes, our ability to better help the near-visually challenged is very evident. Not long ago we had no choices. In this aging population, presbyopia correction will be the single largest area of growth for refractive surgery patients.
Clinical studies are attempting to determine the effectiveness of corneal inlays, nomograms to create presbyopic correction on the corneal surface, and use of a femtosecond laser to treat within the cornea. Bausch + Lomb has developed the Femtec laser to perform IntraCor. This femtosecond laser works within the stroma to correct 1.00D to 1.50D of presbyopia within emmetropic patients. Early in their clinical trials, researchers are using a series of small concentric cuts within the stroma to create a central steepening with smooth transition zones. This creates an increased depth of field and provides both distance and near vision in the eye. This same phenomenon has been observed with hyperopic LASIK patients who have induced negative spherical aberration.
Similarly, this is the rationale behind a new technique termed progressive multifocal LASIK (PML), developed by Roberto Pinelli in Brescia, Italy. PML, used off-label with either the Technolas (B&L) or Wavelight Allegretto Laser (Alcon), may provide another surgical option for our near-challenged patients. Data from the Gordon & Weiss Vision Institute with 214 patients reporting after three months indicate that 86 percent of the patients achieved better than 20/20 uncorrected distance visual acuity and 95 percent of the patients read better than J3.
Cataract surgery as a refractive technique is a mindset that eyecare professionals have adopted quite easily. Patients do not want to wear glasses after surgery, and they should not be required to if they do not desire them. The lens-challenged patient is also entitled to the safest surgical procedure. For years patients have been inquiring about how the surgery will be performed, and their notion has always been that it's performed with a laser. Life was simple when we could just say "No, it is sound waves that emulsify the lens."
However, those days may be coming to an end with the introduction of the femtosecond laser for cataract surgery. LenSx Lasers, Inc. (recently acquired by Alcon) has initiated clinical trials on a femtosecond laser to perform cataract surgery. The laser will initially create a surgical incision in both dimension and architecture, a centered and sized cap, as well as liquefy, soften, and chop the natural crystalline lens. Thus the ultimate goal would be to shift a manual, multistep, and multitool procedure to one laser with surgeon-controlled precision. Early in the clinical trials, we've seen accuracy within <+0.25mm of the diameter of the capsulotomy. No radial tears have been reported; no adverse events and complete removal of the capsule.
In my practice, we have seen the average age of cataract surgery patients fall to approximately 62 years old. It is not difficult to envision that this is initiated from the desire to improve quality of vision. However, it is also a manifestation of refractive surgical outcomes. Essentially, glasses, especially reading glasses, are the harbinger of old age. Cataract surgery in the year 2010 has to be considered a refractive procedure and treated as such. The removal of the lens is a definite method to assuage a middleage hyperope's or high myope's refractive angst.
The three FDA-approved lenses for presbyopic correction continue to be adopted at a quick pace. The recently released Crystalens AO (B+L, Figure 5) has an aspheric front surface with a large 5.0mm optic zone diameter. It is the only true accommodating IOL lens, using accommodative arching to induce negative spherical aberration and shorten the near focal point. The single focality of this lens, combined with the aspheric surface, reduces the risk of glare and haloes. Patients can expect a near focal improvement with exceptional distance vision.
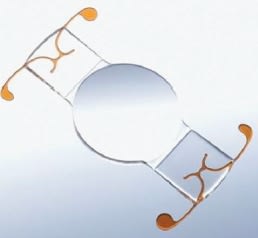
Figure 5. Bausch + Lomb's Crystalens AO is the only true accommodating intraocular lens.
The two available diffractive lenses have also been augmented in this past year. Alcon realized that the ReStor 4.0 near focal point of 3.20D compromised patients' intermediate abilities. Therefore, the ReStor 3.0 is equipped with a spectacle plane add of 2.50D within the same 3.6mm apodized diffractive area. The ReStor 3.0 is manufactured with Alcon's distinctive yellow AcrySof material and has the aspheric anterior optic. In addition, AMO's Tecnis Multifocal IOL (Figure 6) has an anterior aspheric surface with a full diffractive posterior surface. Replacing the ReZoom lens, the Tecnis provides the advantage of a full diffractive, versus a partial, and is therefore considered pupil-independent. As younger patients are opting for refractive surgery, the average pupil diameter is larger than in years past. It is evident that pupil diameter is critical when making clinical decisions.

Figure 6. AMO's Tecnis MF has an anterior aspheric surface with a full diffractive posterior surface.
Make an Effort to Embrace New Technologies
All procedures have early adapters, and thus we may see patients who are not performing as well as designed. It is important to never stop looking for refractive solutions for dissatisfied patients. I have attempted to avoid offering no solution. Rather, I have opted for a work-in-progress mentality and providing an optimistic "eye" on the future. This outlook has proved fruitful with some new developments in corneal treatment. Ironically, some older procedures can be recycled to help with unwanted visual sequelae.
Eyecare professionals should be quick to consider new technology. Removing this refractive surgery myopic view will help us to advance and educate on new procedures. This is typified in the use of Intacs (Addition Technology) for the correction of keratoconus. Originally designed to treat low myopic correction without removing tissue from the central cornea, these cylindrical PMMA segments have been successfully inserted in keratoconic (and ectatic) patients. As reported by Dr. Marlane Brown at the Optometric Council on Refractive Technology symposium in 2009, 25 eyes with keratoconus or ectasia were treated with Intacs and conducive keratoplasty at Minnesota Eye Consultants. Dr. Brown stated that 80 percent currently tolerate spectacles or contact lenses with an average of 16 months of follow-up care. It is important for us to convey this information to our patients.
Another promising refractive process pertains to strengthening the stroma of the cornea. Clinical trials are being conducted on the infusion of riboflavin 0.1% into the corneal stroma with a UV-X light source to create a corneal cross-link. The use of cross-linking (CXL) can then create a more stable cornea in keratoconic, ectatic, and post-RK eyes. CXL (otherwise known as C-3R) may be a procedure that optometrists can and should embrace because of its non-invasive nature.
Dr. Brian Boxer-Wachler used the same technique combined with a Visian lens to decrease the visual impairment of an American Olympic gold medal bobsledder who participated in the 2010 Winter Olympics. This exemplifies the ability to think outside the box, combining different new refractive procedures to elicit an unforeseen refractive outcome.
The advances in technology do not necessarily entail adding new procedures, rather we are observing the existing surgeries improving. It was not that long ago that I personalized music cassettes by sitting next to the radio and waiting to push "record" when I heard my song pop up. Now I can plug a mini-computer into the World Wide Web and instantaneously create a play list of my favorite tunes. This is analogous to your patients who, not that long ago, would eliminate their need for glasses or contact lenses by having a surgeon manually place a blade into 80 percent of the depth of their cornea. The quality and effectiveness were not always great. But today we can prepare the eye, limit unwanted sideeffects, and use laser technology to reshape patients' vision. What a great time to consider undergoing refractive surgery. CLS
To obtain references for this article, please visit http://www.clspectrum.com/references.asp and click on document #178.